Term "anti-vaxxer"
is a propaganda ploy
Actual science conflicts with
pharmaceutical industry-promoted hysteria
By James Richard Bailey
INTRODUCTION:I'm going to go ahead and start putting news into the beginning of this article regarding the Covid-19 pandemic. It is just too important to address the issues at hand. That being said, the information in the rest of this article is still scientifically solid.
To begin with, let's differentiate between the virus, SARS-CoV-2 and the collection of symptoms (i.e. syndrome) labeled Covid-19. The virus is in the family of Coronaviruses that has been around since before humans evolved into homo sapiens. In all those millenia, no severe disease has been the result of a Coronavirus infection. The most recognized manifestation is the common cold.
Only in the last couple of decades has the pathogen ever been deadly. Coincidentally, this has only taken place since the US Centers for Disease Control and Prevention received a patent on it and undertook to enhance its deadly nature through gain-of-function experimentation.
For now, I will present the best information available regarding preventive nutritional measures that can be taken by the public short of the experimental "vaccines" being foisted upon us. A combination of vitamin D3, zinc and vitamin C is recommended.
In this review, the role of zinc, vitamin C and vitamin D for immunity was explored since these micronutrients show the strongest evidence for immune support. In this scenario, the mentioned studies demonstrate that zinc and vitamins C and D are integral parts of the immune system and show synergistic functions at various stages of a host's defenses, such as the maintenance of the integrity of biological barriers and the functionality of cells that make up the innate and adaptive systems. Therefore, the deficiency or insufficiency of these key nutrients, acting in synergy in tight and adherens junction proteins, can lead to impairment of mucosal epithelial cells, possibly making them more susceptible to pathogen entry, such as SARS-CoV-2.
____________________original 2017 article starts below this line____________________________
The public discussion about vaccines has recently escalated to the level formerly occupied by the Ebola virus. I'm a media analyst who pays particular attention to whichever media circus is currently in vogue. Whether it is war, or terrorism, or disease, there is always some fear mongering specialty of the day going on.
♦ If the text is too small and hard to read, use your browser's View menu to Zoom In ♦
Currently, it is has to do with measles outbreaks in the good old U.S.A. Nothing big, mind you. No serious medical complications, no deaths. Just measles outbreaks. Yes, the United States experienced a small number of measles cases during 2014, with 644 cases from 27 states reported to CDC's National Center for Immunization and Respiratory Diseases (NCIRD). That was an unusual year. In 2013 there were 187 cases reported, and in 2015, there were 188 people reported to have had measles. Contrary to the impression given by scientifically illiterate talking heads, the number for 2016 was down to just 70 cases, less than half that of the previous year.
From these figures, the pro-vaccine fanatics are claiming that 2014 saw a record number of measles cases. Examine the claims more closely, and you'll find that is only a record for the 21st Century, since measles was declared eradicated in 2000. It is a far cry from the early decades of the 20th century, when thousands of fatal measles infections were reported each year. During the 1950s an annual average of greater than 500,000 cases of measles and nearly 500 deaths blamed on measles were reported in the United States. Surveys indicated that 95% of the population had been infected with measles by the age of 15 years. Note that the following link from 1983 predicted the elimination of measles "entirely from the country within the year". http://www.ncbi.nlm.nih.gov/pubmed/6878996
Measles deaths actually due to pneumonia
What you won't find reported is the fact that those fatality numbers had plunged to a small fraction before vaccinations began. This was due mostly to improved sanitation and nutrition, as well as common advances in medicine including the development of antibiotics. One wonders where is the media reporting on the fact that the overwhelming number of measles deaths were due to pneumonia. Very few people know that measles is actually a respiratory disease. Transmission of this infection is most often attributed to airborne, cough-expelled droplets. The first sign of measles is a sore throat and a cough. Pneumonia, of course, is easily treatable with antibiotics.
Vaccines are dangerous
Vaccines can injure or even kill. That is why all US vaccine manufacturers are protected from law suits and criminal prosecution. To understand how this happened, we have to turn the clock back to 1982, when Big Pharma blackmailed Congress. That is when four big drug companies (Merck, Wyeth, Lederle, Connaught) threatened to stop selling vaccines in America unless a law was passed giving them complete immunity from prosecution.
The pharmaceutical industry knew they were in big trouble because the old, crude whooping cough vaccine in the DPT shot was causing brain inflammation and death in many children. The live oral polio vaccine was crippling children and adults with vaccine strain polio; and Americans were filing lawsuits to hold drug companies responsible for the safety of their products. So, the manufacturers demanded to be shielded from liability.
The companies' ploy worked, and on Nov. 14, 1986 President Reagan signed the National Childhood Vaccine Injury Act. It provided for a system that would be administered by the Federal judiciary to compensate those with provable claims. At the same time, it was guaranteed under the same law that parents would still have the ability to sue the companies if their claims were denied by the federal system. The law had, after all, been set up so that 2/3 of applicants were denied. Furthermore, compensation for a death resulting from vaccination was capped at $250,000.
US Vaccine Court has paid out billions of dollars
If you need positive proof that vaccines are much more dangerous than your doctor says they are, here it is. The U.S. Vaccine Court paid out $4 BILLION DOLLARS in damages to people who have been injured by vaccines from 1988 through 2018.
What, you didn't know there is a U.S. Vaccine Court? Well, there is. And no, that isn't its real name. Vaccine Court is the popular term which refers to the U.S. Court of Federal Claims Office of Special Masters, which administers a no-fault system for litigating vaccine injury claims.
In 1986, Congress created the Vaccine Injury Compensation Program (VICP) under the National Childhood Vaccine Injury Act. This program has original jurisdiction for children's claims of vaccine injury.
The VICP has compensated approximately 2,500 claims [link to study] of vaccine injury since the inception of the program. A study of these claims found 83 cases of acknowledged vaccine-induced brain damage that include autism, a disorder that affects speech, social communication and behavior. In 21 published cases of the U.S. Court of Federal Claims Office of Special Masters, which administers the VICP, the Court stated that the petitioners had autism or described autism unambiguously. In 62 remaining cases, the authors identified settlement agreements where Health and Human Services (HHS) compensated children with vaccine-induced brain damage, who also have autism or an autism spectrum disorder.
This finding of autism in compensated cases of vaccine injury is significant. U.S. government spokespeople have been asserting no vaccine-autism link for more than a decade. This finding calls into question the decisions of the Court of Federal Claims in the Omnibus Autism Proceeding in 2009 and 2010 and the statement of Health and Human Services on its website that HHS has never concluded in any case that autism was caused by vaccination.
Using publicly available information, the investigation shows that the VICP has been compensating cases of vaccine-induced brain damage associated with autism for more than twenty years. This investigation suggests that officials at HHS, the Department of Justice and the Court of Federal Claims may have been aware of this association but failed to publicly disclose it.
Overview
From my research into this topic, I have come to the following conclusions:
-
While there are Autism Spectrum Disorders (ASD) sometimes caused by the MMR vaccine, many other disorders, and even deaths, are also caused by virtually all vaccines, a proposition that is proven by decisions of the Vaccine Court and subsequent awards of compensation.
-
Vaccines are not nearly as effective as claimed, and they even contribute to outbreaks by causing the very disease that they are supposed to prevent. It can be shown that decline in disease rates is due to advances in public health,
-
Serious complications of measles are preventable with administration of vitamins A and C in pharmacological doses, supporting the conclusion that in and of itself, measles need not be thought of as a horrible malady. Similar effects of vitamin C are applicable to whooping cough. Complications are also due to malnutrition and other factors such as parasitic infection and reduced resistance from other stressors like dehydration, chemical toxicity and exhaustion.
-
The option of informed consent is not presented as a consideration to patients or, if they are children, to their parents. There are moral rights to informed consent, and the legal choice to decline the vaccination intervention.
-
Herd immunity is entirely different from the common explanation given in the media.
-
The increase in the number of vaccines, and the early age at which they are routinely administered causes many disorders.
-
The immunity imparted by natural means is far superior to that acquired through the use of vaccines. (i.e. cell mediated immunity versus antibody based immunity)
-
Additives in manufactured vaccines are highly toxic.
-
As publicly perceived, the risk benefit analysis involved in the choice to vaccinate is largely skewed.
-
The profit motive of pharmaceutical companies is the main reason new vaccines are developed and promoted.
-
There is a joint effort of corporations and government to cover up these facts. There is corruption in the CDC, and conflicts of interest in medical journals, contributing to ignorance about and prejudice in favor of vaccination intervention on behalf of medical doctors.
-
Propaganda regarding vaccine resistance shows a consistent thread that ignores scientific and legal data, and which paints vaccine resistance as emotional, ignorant and superstitious. At the same time, propaganda in favor of vaccinating is full of dishonesty and logical faults. Andrew Wakefield, MD is the favored target of ad hominem attacks, and he was wrongly persecuted by prominent persons in collusion with vaccine manufacturers.
(1) Vaccine Court: The proof is a matter of public record
In 1955 about 200 people were paralyzed and 10 died after contracting polio from the Salk polio vaccine. Through the 1970s and 1980s, the number of lawsuits brought against vaccine manufacturers increased dramatically, and manufacturers made large payouts to individuals and families claiming vaccine injury, particularly from the combined diphtheria-pertussis-tetanus (DPT) immunization.
That is why in 1986 the industry was protected from further liability by the National Childhood Vaccine Injury Act, which led to the inception of the Vaccine Injury Compensation Program (VICP) and the Vaccine Adverse Events Reporting System (VAERS).
I said from the beginning that our government has confirmed in a Federal court of law that vaccines cause injuries. I first present the landmark case of a child who rapidly regressed and became autistic after a round of routine childhood vaccinations.
This case involved 10 year old Ryan Mojabi of California, in which the government admitted that the MMR vaccine caused the brain encephalopathy or brain dysfunction Ryan suffered within five to fifteen days of receiving the shot. Encephalopathy is considered a vaccine table injury, in other words, a compensatable adverse reaction to vaccination. Seizures, spiking fevers, a measles-like rash of red spots all over the body, and ultimately brain encephalopathy were reported following the shots. The witnesses said that he never fully recovered from the adverse vaccine reactions they experienced, losing eye contact, language, and social skills, all hallmark symptoms of autism. Because it was proven in a federal court that Ryan Mojabi suffered from an effect of the vaccine that lead to encephalopathy, he was awarded A lump sum payment of $969,474.91
The point here is that autism was caused by the encephalopathy, which was caused by the vaccines. I am not saying that all autism is caused by vaccines. That is a bit of specious pseudo reasoning that is used as a straw man by apologists for the vaccine manufacturers and holders of the outdated paradigm within the medical community.
There is a lot of that sort of poppycock going around. It's just like certain bloggers who say that decisions made by the VICP don't prove anything scientifically. That is true. These decisions only prove that a particular injury followed a vaccination episode. The Mojabi case was successfully prosecuted in an extremely difficult legal system that discards the vast majority of cases before they even start. Not that Steven Novella, creator of Skeptical Science, would acknowledge such a distinction.
In a system designed to shield vaccine manufacturers from liability for injuries caused by their products, Ryan B. Mojabi was awarded $969,474.91 in 2012. Again, apologists for the manufacturers say "This is money that came out of a tax on the manufacturers. They were not sued in a court of law."
No kidding. That is because, by rule of law, it is not possible to sue the manufacturers. The whole system in the US Court of Federal Claims protects them from that! To get a feel for the propaganda being fed to the general public, read the common defense put forth in the web site Skeptical Science. Titled Anti-vaccine kooks still at it, it is full of claims that stand unsupported by fact. They make it seem as if suffering and death from infectious diseases are common, and that adverse effects from the vaccines are rare...exactly the opposite of the truth! I would expect no less from Steven Novella, the website's creator.
Vaccines are dangerous. That we know from the proceedings of the Vaccine Court. From these we learn that the influenza vaccine is the most dangerous vaccine of all, based on the percentage of settled cases.. Here is a window into that statistic.
From August 16 to November 15, 2013, there were 139 claims settled, with 70 of them being compensated by cash awards. Of the 70 cases compensated, 42 were for injuries or deaths linked to the influenza vaccine. That is 60%. The combined total of the other 40% of cases settled included the following vaccines: Hep B, Tetanus, HPV, DTaP, MMR, IPV, PCV, Hib, Meningococcal, Varicella, and TD.
During that time the Vaccine Court paid almost $64 million [$63,796,836.] as compensation for 70 claims. Let that sink into your mind. In just one quarter of the year 2013 that much money was paid out to 42 claimants of vaccine injury.
(2) Many vaccines are ineffective and can actually cause disease
Statistics are always interpreted and presented in such a way as to make it appear that vaccines are foolproof in their effectiveness. One such claim is that the MMR vaccine protects kids from death, based on statistics that actually make the opposite case. Look at this chart, showing the mean annual mortality cases in England and Wales from 1900 until the MMR vaccine was introduced. Mortality was reduced through better treatment of disease complications.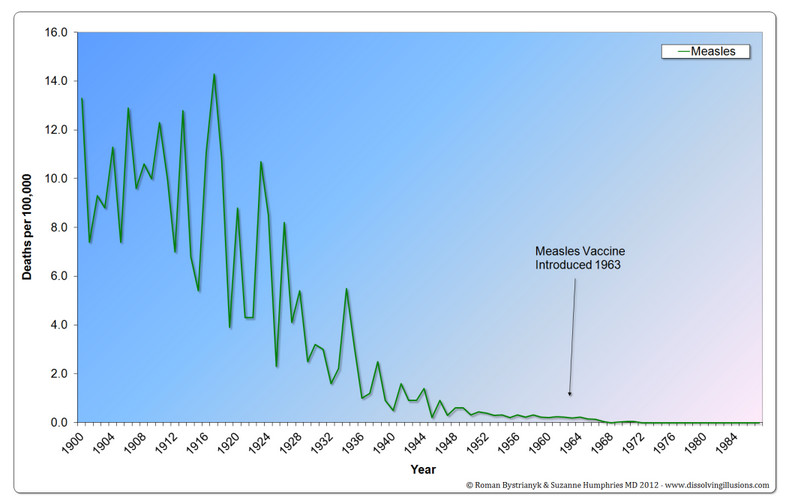
When vaccines for childhood diseases were introduced, they were touted as providing lifetime protection, just like natural immunity. It was then learned that their effectiveness only lasted from 2 to 10 years, after which booster shots were needed. Soon afterward it became apparent that the booster shots themselves only lasted one or two years. Now we are told that in order to provide lifelong protection, we must have booster shots throughout our lifetimes.
Another claim is that while vaccines do not guarantee complete protection from a disease, they are generally very effective for most. The qualifiers in that statement are "complete protection" and "generally effective for most". Semantically speaking, nothing provides complete protection from anything. Moreover, general effectiveness is so much puffery.
Let's look at protection and effectiveness of various vaccines from a couple of angles.
Pertussis (whooping cough)
During recent outbreaks, the majority of whooping cough cases were among the population of fully vaccinated people, not in those who were unvaccinated.
In the US, from January 1 to June 16, 2014, there have been nearly 10,000 cases of pertussis, or whooping cough, confirmed by the US Centers for Disease Control and Prevention (CDC). This is a 24 percent increase compared to the same time period in 2013. The CDC maintains that the best way to prevent pertussis is to get vaccinated, but this deserves a closer look.
Fully vaccinated children may still get whooping cough, and at very high rates. During the recent outbreak of whooping cough in California, 81% of the victims were fully vaccinated, and 11% were partially vaccinated. Contrast that with this: only 8 percent of the afflicted patients were unvaccinated. Researchers noted the vaccine's effectiveness was only 41% among 2- to 7-year-olds and a dismal 24% among those aged 8-12.
In a study published in the Oxford Journal of Clinical Infectious Diseases, researchers reviewed data on every patient who tested positive for pertussis between March and October 2010 at the Kaiser Permanente Medical Center in San Rafael, California. Out of these 132 patients:
-
81 percent were fully up to date on the whooping cough vaccine
-
8 percent had never been vaccinated
-
11 percent had received at least one shot, but not the entire recommended series
The amount of protection remaining after 5 years depends heavily on the initial effectiveness. If the initial effectiveness of DTP was 90%, it would decrease to 42% after 5 years. Regardless of the initial effectiveness, the protection from disease afforded by the fifth dose of D Tap among fully vaccinated children who had exclusively received D Tap vaccines waned substantially during the 5 years after vaccination.
The pertussis (whooping cough) vaccine is included as a component in "combination" shots that include tetanus and diphtheria (DPT, DTaP, Tdap) and may also include polio, hepatitis B, and/or Haemophilus Influenza B (Hib). CDC data shows 84 percent of children under the age of three have received at least FOUR DTaP shots ”which is the acellular pertussis vaccine that was approved in the United States in 1996” yet, despite this high vaccination rate, whooping cough still keeps circulating among both the vaccinated and unvaccinated.
Here is one way that the effectiveness of vaccines is exaggerated through collusion between governmental health organizations and manufacturers. In the April, 2012 issue of Pediatrics a doctor from the World Health Organization stated that "Our estimates of vaccine efficacy [effectiveness] have been inflated because of case definition." He was on the WHO committee that did the standardized tests on the whooping cough vaccine.
That doctor, James D. Cherry MD, MSc, said that the whooping cough vaccine is at best only 40% effective, not 84% as vaccine manufacturers claim. READ FULL STATEMENT HERE, PDF DOWNLOAD
The acellular pertussis vaccine, like all vaccines, does not confer lifelong immunity. The first shot gives 41% protection among 2- to 7-year-olds, and a dismal 24% among those aged 8-12. Those percentages decline by 10% a year.
Keep in mind that after having contracted whooping cough, one has natural immunity the rest of one's life. Contrast that with vaccine acquired immunity, which must be renewed with a booster shot every few years the rest of one's life.
"We've had over 90% baby vaccination rates for whooping cough vaccines for over 11 years since 2000, AND they've included even more shots since then for the adolescents at the time, and yet more, after 2000, AND here we are with whooping cough in EVEN higher numbers than it was before 1960? Don't you think that's absolutely astonishing? Australia, which has had over a 95% whooping cough vaccination rate since 2000, is having the largest outbreak in their history since pertussis vaccination started. The same is happening in USA, and their rate of vaccination is even higher than Australia. So what do you think is happening there?" Hilary Butler
[In Wisconsin, 2004] We identified 261 pertussis cases among county residents; 149 (57%) were laboratory confirmed. Of the first 57 case patients, 47% reported using a particular high school weight room. Pertussis incidence was high in all age groups; 86% of case patients were 10 years or older. Among 156 case patients with reported vaccination histories, 84% had received 5 or more doses of pertussis-containing vaccine. Adults reported significantly more severe pertussis symptoms than adolescents. LINK
Doctors have begun encouraging adults to get a pertussis booster if it has been more than a decade since their last shot. Physicians also now urge adults who spend time around infants to get a booster, since the disease can be devastating to babies.
Mumps
Did Ineffective MMR Vaccine Promote Mumps Outbreaks? Dangers of vaccines reported, but reports buried by lies and deception.
In 2009, more than 1,000 people in New Jersey and New York came down with mumps. A similar scenario occurred in 2006, when mumps infected more than 6,500 people in the US. Most of those cases also occurred among the vaccinated population, primarily among college students who had received two doses of . "Why did the majority of outbreaks occur in areas that are thought to HAVE herd immunity status, i.e. where the majority of people are vaccinated and "should" therefore never get the disease.
Philadelphia outbreak deaths were preventable if the religiously constrained parents would have taken their children to the hospital as soon as symptoms of encephalopathy and/or pneumonia had presented themselves.
According to these two lawsuits, Merck began a sham testing program in the late 1990's to hide the declining efficacy of the vaccine. The objective of the fraudulent trials was to "report efficacy of 95 percent or higher regardless of the vaccine's true efficacy." This program was initially referred to as "Protocol 007," the Chatom claim states, and instead of testing the vaccine's efficacy against a wild mumps virus, as is the norm, Merck used its own attenuated strain of the virus, the identical strain with which the children were being vaccinated!
Merck also added animal antibodies to blood samples to achieve more favorable test results, though it knew that the human immune system would never produce such antibodies, and that the antibodies created a laboratory testing scenario that "did not in any way correspond to, correlate with, or represent real life ... virus neutralization in vaccinated people," according to the complaint. [FROM MERCOLA]
Outbreak in 2009, nearly all had been vaccinated
In 2009, more than 1,000 people in New Jersey and New York came down with mumps. At the time, questions arose about the effectiveness of the vaccine as 89 percent of those sickened were vaccinated. About 3,502 children of primarily Orthodox Jewish upbringing developed mumps between June 28, 2009, and June 27, 2010, as a result of an unusual "face-to-face" educational method used at certain all-boys Jewish schools throughout the New York and New Jersey areas. Among those affected by the outbreak, 97 percent were said to be Orthodox Jewish persons, and nearly one-third were between the ages of 13 and 17.
After confirming 1,648 cases of infection using clinical specimens, the research team that compiled the study determined that 89 percent of all those who contracted mumps as a result of the outbreak had already been vaccinated at least twice for mumps, presumably with the controversial measles, mumps, and rubella (MMR) combination vaccine that has been implicated in causing gastrointestinal disorders and autism. Another eight percent of the group had reportedly received only one dose of the mumps vaccine, meaning that 97% of the stricken had been vaccinated.
Learn more: http://www.naturalnews.com/038554_mumps_outbreaks_vaccinations_children.html#ixzz3gNwRlScz
Influenza
The influenza vaccine has the worst effectiveness record of all. The US Centers for Disease Control and Prevention (CDC) estimated the effectiveness of the vaccine for the 2014-15 flu season at 19%. In the past three flu seasons, the flu vaccine's effectiveness has been touted as being between 47% and 62%, while some experts have put it as being between 0% to 7%. This qualifies as an EPIC FAIL! Similarly, in the flu season of 2003-04 completely missed the mark, with official CDC estimate of effectiveness at 3% to 14%. Furthermore, these were official estimates which we can assume erred on the side of the pharmaceutical industry.
It is important to realize that influenza often mutates, and the strains that make the rounds in any given year are always different. This is a huge problem for the manufacturers of vaccines, who must have their products ready for market each year in early autumn. The US Food and Drug Administration's (FDA) Vaccines and Related Biological Products Advisory Committee selects the different influenza strains each year that manufacturers should include in their vaccines for the U.S. population for the upcoming influenza season. The closer the match between the circulating strains causing disease and the strains in the vaccine, the better the protection against influenza.
But, the selection process is at best hit-and-miss. The influenza viruses selected for inclusion in the seasonal flu vaccines are updated each year based on which influenza virus strains are circulating, how they are spreading, and how well current vaccine strains protect against newly identified strains. Five World Health Organization (WHO) centers (US, Great Britain, Australia, Japan and China) collect information from 111 countries around the world. WHO then recommends specific viruses for inclusion in seasonal vaccines, and then individual countries decide which ones to license in their domain.
In the US, the FDA decides which strains are to be included in vaccines licensed for use here. All of this is done six months to a year before the vaccines are produced, and it often amounts to little more than guesswork. The result is the aforementioned dismal success rate.
Worse even than the lack of effectiveness is the rate of officially compensated injuries caused by the flu shots. The June 15, 2014 report from the US Vaccine Injury Compensation Program covering just a three-month period shows that the flu vaccine is the most dangerous vaccine in America. There were 78 cases awarded settlements for injuries from all types of vaccines, with 55 of the settlements being for the flu shot, including one death. WHY IS THIS STUNNING NEWS NEVER REPORTED BY OUR MASS MEDIA?
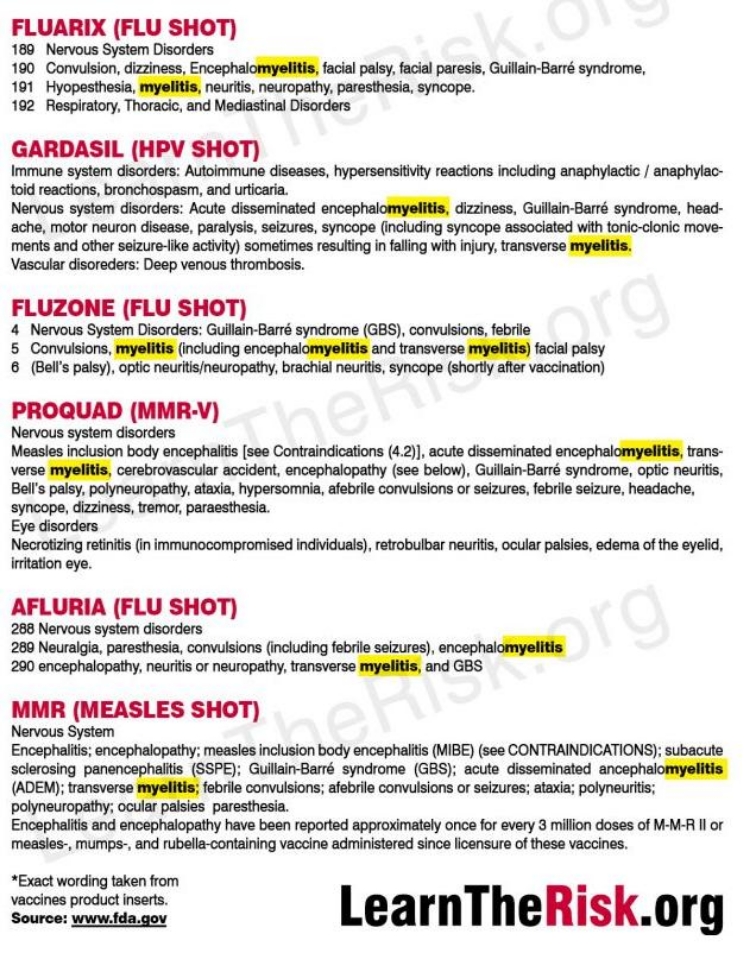
Most of the settlements for injuries due to flu shots were for Guillain-Barré Syndrome. Other flu vaccine injuries included chronic inflammatory demyelinating polyneuropathy, rheumatoid arthritis, shingles, brachial plexus neuropathy, Bell's Palsy, brachial neuritis, transverse myelitis, lichenoid drug eruption and narcolepsy.
Can the flu shot actually give you influenza? The quick answer is YES.
Flu shots CAN actually give a person influenza. (warning, science alert) It works like this. The flu vaccine contains either "attenuated" (weakened), or killed, flu viruses. They are supposedly weakened or killed by the inclusion of formaldehyde in the vaccine formula. The problem is, that formaldehyde doesn't always do the job. Hence, some live viruses get included in some batches of flu vaccine. Furthermore, sometimes the non-killed viruses mutate into different, or even more virulent, viruses. NOTE: THE FOLLOWING IS FROM A SCIENTIFIC JOURNAL. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4353909/
An explanation of the above article more suitable for us non-scientists can be found HERE.
Tetanus
'Tetanus is caused by an infection with the Clostridium tetani bacterium. The bacteria generally enter through a break in the skin such as a cut or puncture wound by a contaminated object. The bacteria are commonly found in soil, dust and manure. The bacteria produce toxins that interfere with muscle contractions, resulting in the typical symptoms. Diagnosis is based on the presenting signs and symptoms. The disease does not spread between people.“ Wikepedia
Tetanus (a.k.a. lockjaw) is a disease of the past unless one lives in a third world country or is horribly injured in war and left untreated. The tetanus bacteria are present in the gut of most mammals, but do not cause disease.
The effectiveness of tetanus toxoid has never been studied in a vaccine trial, according to the CDC. Furthermore, tetanus is not transmissible from person to person. It can only be contracted through spores that are everywhere in the environment. Soil and dust! Yet it is one of three vaccines that are components of the standard DTaP inoculation.
Although a major disease in tropical under-developed countries, tetanus in the USA has been very rare. In the past, tetanus occurred primarily in poor segments of the population in southern states and in Mexican migrants in California. It was swiftly diminishing with each decade prior to the 1950s (in the pre-vaccination era), as inferred from tetanus mortality records and similar case-fatality ratios (about 67-70%) in the early 20th century versus the mid-20th century). The tetanus vaccine was introduced in the USA in 1947 without performing any placebo-controlled clinical trials in the segment of the population (children or adults), where it is now routinely used.
The rationale for introducing the tetanus vaccine into the U.S. population, at low overall risk for tetanus anyway, was simply based on its use in the U.S. military personnel during World War II.
According to a post-war report: in World War One there were 70 cases of tetanus among approximately half a million admissions for wounds and injuries, an incidence of 13.4 per 100,000 wounds. In World War Two there were almost three million admissions for wounds and injuries, with a tetanus case rate of 0.44 per 100,000 wounds.
The report leads us to conclude that vaccination has played a role in tetanus reduction in wounded U.S. soldiers during WWII compared to WWI, and that this reduction vouches for the tetanus vaccine effectiveness. However, there are other factors (e.g. differences in wound care protocols, including the use of antibiotics, higher likelihood of wound contamination with horse manure rich in already active C. tetani in earlier wars, when horses were used by the cavalry, etc.), which should preclude us from uncritically assigning tetanus reduction during WWII to the effects of vaccination. READ MORE
For a wonderful presentation on this topic, view this 45 minute VIDEO by Dr. Suzanne Humphries M.D.
Chicken pox
According to Merck's own package insert, 4% of children getting the chicken pox vaccine actually contract the disease from it. Of course, they refer to it as a "varicella-like rash". Furthermore, persons receiving the vaccine can transmit chicken pox to others even though they don't show symptoms themselves. This too is in their package insert. (pdf link).
Of equal or greater importance is the fact that having chicken pox creates natural immunity to the herpes virus which, in turn, protects us from shingles. Vaccine induced antibodies don't do that, which has contributed to the greatly increased incidence of shingles in the general population. (pdf link) From International Journal of Toxicology
Between March 1995 and July 1998, the federal Vaccine Adverse Events Reporting System (VAERS) received 6,574 reports of health problems after chickenpox vaccination. That's one adverse health event for every 1,481 chicken pox vaccinations, 14 of which resulted in death. As a result of these vaccine reactions, 17 warnings were added to the manufacturer's product label after the vaccine was being used.
It's worth mentioning that adverse vaccine events are greatly under-reported (by as much as 90 percent, according to some experts) making the dangers of the chicken pox vaccine possibly far worse than these statistics imply.
Measles
Dr. Ronald Penny, associate professor of medicine at St. Vincent's Hospital in Sydney in an interview,(Australian news magazine (The Age, April 12, 1975) that a number of children were regularly harmed or killed by vaccinations, and that they were most likely to be children who had deficiencies in their immune systems.
According to Dr. Penny, measles, rubella, and polio inoculations were the most dangerous because they involved live viruses. He explained that weakened viruses are in the vaccines; but, placed in a person with a weak immune system, they are as dangerous as a vigorous set of germs placed in a healthy person.
Measles vaccine was originally touted as providing lifetime immunity to the disease. By 1989, because of numerous issues “including the determination that the older vaccines were not widely effective“ everyone under the age of 32 (anyone born after 1957) was urged to be revaccinated.
In 1997, Miller notes that, "When the measles vaccine was introduced in 1963, officials were confident that they could eradicate the disease by 1967."
Subsequently, new dates for eradication were pronounced as 1982, 2000 and 2010. Meanwhile, in 1990, after examining 320 scientific works from around the world, 180 European medical doctors concluded that "the eradication of measles would today appear to be an unrealistic goal." And in 1984, Professor D. Levy of Johns Hopkins University had already concluded that "if current practices [of suppressing natural immunity] continue, by the year 2050 a large part of the population will be at risk and there could in theory be over 25,000 fatal cases of measles in the U.S.A."
Polio
Polio was not conquered by vaccines. Epidemics of polio were stopped by proper plumbing. The following is from HERE "Polio thrives in fecal matter and is easily transmitted through human waste. In areas where sanitation and hygiene are good, polio is rare. In areas where sanitation and hygiene are poor, the disease can spread rapidly. India is the second most populous nation in the world, with an estimated population of 1.2 billion. Currently, 780 million Indians do not have a toilet; 96 million Indians do not have access to clean drinking water. In rural areas, open defecation is still more common than attempting to dispose of human waste in a more sanitary fashion, such as burying it.
"There have been some efforts to improve sanitation, but they pale in comparison to the extensive efforts to vaccinate Indians. Over 9 billion has been spent in this vaccination public health campaign. In some parts of India, children have received as many as 30 doses of the oral polio vaccine before their fifth birthday. Bill Gates, the World Health Organization, and GAVI have ardently been pushing vaccines on people who still don’t have access to clean drinking water or the sanitary means to dispose of human waste.
"The current polio vaccine campaign in India is highly controversial due to the high rate of vaccine injury and death. There were 53,000 cases of NPAFP, a non-polio acute flaccid paralysis, among those vaccinated. NPAFP is a disease that is clinically indistinguishable from polio and twice as deadly that is caused by the live, weakened, polio viruses in the vaccine. Incidences of the disease rose and fell with the number of doses of the vaccine administered. To call this disease anything other than polio is semantic subterfuge, a whitewash for Big Pharma’s image.
In the past 13 months, India has reported 53,563 cases of NPAFP at a national rate of 12 per 100,000 children—way above the global benchmark set by WHO of 2 per 100,000.” – Jan, 13 2014 quote from LiveMint Newpaper, the second largest business newspaper in India."
The United States of America is seeing acute flaccid myelitis quickly spreading through most states. IT IS NOT KNOWN TO BE CONTAGIOUS. Is the "mystery" of paralysis really such a "mystery"? It's listed as a side effect of vaccines. This is from <learntherisk.org>.
From August 2014 to September 2018, the CDC received reports of 386 confirmed cases of AFM in the U.S. Broken down, this amounts to:
- 62 confirmed cases so far in 2018 (as of October 16), spread across 22 states
- 33 confirmed cases in 2017, across 16 states
- 149 confirmed cases in 2016, across 39 states
- 22 confirmed cases in 2015, across 17 states
- 120 confirmed cases from August to December 2014, across 34 states
It should be noted that the CDC is currently investigating nearly 130 possible AFM cases with onset of symptoms in August and September 2018. The 62 confirmed cases for 2018 are among these reports, but it's possible the number may rise considerably in the coming months. LINK
Sabin's live virus oral polio vaccine is capable of causing polio in some recipients of the vaccine, and in individuals with compromised immune systems who come into close contact with recently vaccinated children who will be shedding enough of the vaccine to infect anyone around them. As a result, in January 2000, the CDC "updated" its polio vaccine recommendations, reverting back to policies first implemented during the 1950s: Children should only be given the killed-virus shot. The oral polio vaccine should only be used in special circumstances. [Gorman C. When the vaccine causes the polio. Time October 30, 1995:83]
Virus shedding...how vaccines spread disease
Many of the common vaccines use live attenuated viruses (LAV). This means that the virus that causes the disease, measles for example, is treated with a substance that supposedly make it less virulent. Formaldehyde is one such substance. Measles, mumps, rubella, influenza and chicken pox are common diseases that fall into this category.
Several risks are present in the this method of producing vaccines. Virus shedding is one of those risks. Scientific evidence demonstrates that individuals vaccinated with live virus vaccines such as MMR (measles, mumps and rubella), rotavirus, chicken pox, shingles, smallpox and influenza can shed the virus for many weeks or months afterward and infect the vaccinated and unvaccinated alike.
Outbreaks can be caused by unvaccinated children who were contagious, by vaccinated children who were contagious due to shedding, and by vaccinated children on whom the vaccine had been ineffective. Scientific evidence demonstrates that individuals vaccinated with live virus vaccines such as MMR (measles, mumps and rubella), rotavirus, chicken pox, shingles, polio and influenza can shed the virus for many weeks or months afterward and infect the vaccinated and unvaccinated alike.
The esteemed Johns Hopkins Hospital, for instance, used to warn about virus shedding in its official Patient Guide, urging the immunocompromised to "avoid contact with children who are recently vaccinated." Why? Because the recently vaccinated can, and often do, spread vaccine-derived viruses capable of killing children with weak immune systems.
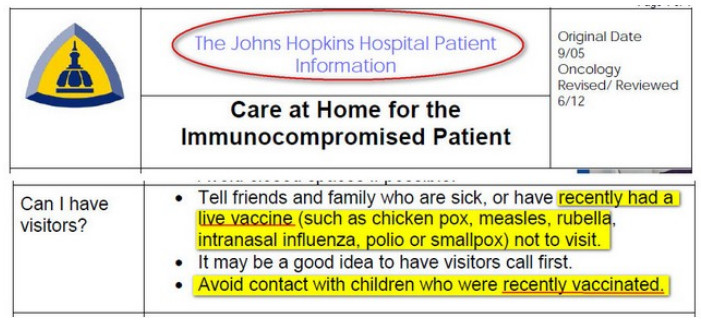
[Author's note: This above graphic was still available through the Johns Hopkins Archive until mid-August, 2015. They have now altered it to leave out the vaccine references. It was formerly available as a pdf HERE. The specific graphic shown was in part 7.d. "Care at Home for the Immunocompromised Patient". The source for this URLwas http://www.thehealthyhomeeconomist.com/studies-show-measles-vaccine-spreads-virus/ After this graphic disappeared, the daveworld.biz website was hacked and brought down in a denial of service attack.
Four types of vaccines are currently available:
-
Live virus vaccines use the weakened (attenuated) form of the virus. The measles, mumps, and rubella (MMR) vaccine, the live oral polio vaccine, and the varicella (chickenpox) vaccine are examples.
-
Killed (inactivated) vaccines are made from a protein or other small pieces taken from a virus or bacteria. The flu vaccine is an example.
-
Toxoid vaccines contain a toxin or chemical made by the bacteria or virus. They supposedly make you immune to the harmful effects of the infection, instead of to the infection itself. Examples are the diphtheria and tetanus vaccines.
-
Biosynthetic vaccines contain man made substances that are very similar to pieces of the virus or bacteria. The Hib (Haemophilus influenzae type B) conjugate vaccine is an example.
Rotavirus...425 deaths associated with vaccine since 2006
Rotavirus is a contagious diarrhea-causing organism that most babies get. Rotavirus is the most common cause of severe gastroenteritis in infants and young children in the United States. The spectrum of rotavirus illness ranges from mild, watery diarrhea of limited duration to severe, dehydrating diarrhea with vomiting and fever. Virtually all children become infected in the first 3-5 years of life, but severe diarrhea and dehydration occur primarily among children aged 3-35 months. Rotaviruses are shed in high concentrations in the stools of infected children and are transmitted by the fecal-oral route, both through close person-to-person contact and through fomites. Rotaviruses also might be transmitted by other modes, such as respiratory droplets.
Rotavirus appears to be responsible for approximately 5%-10% of all diarrheal episodes among children aged less than 5 years in the United States, and for a much higher proportion of severe diarrheal episodes. Although rotavirus gastroenteritis results in relatively few deaths in the United States (approximately 20 per year among children aged less than 5 years), it accounts for more than 500,000 physician visits and approximately 50,000 hospitalizations each year among children aged less than 5 years. [CDC Morbidity and Mortality Weekly Report 3/19/99]
From Vaccine Choice Canada:
Two brands of rotavirus vaccine are currently marketed in Canada. Merck's RotaTeq, is a genetically engineered vaccine containing five human-cow reassortment strains of rotavirus, and GlaxoSmithKline's Rotarix, is a genetically engineered vaccine created by isolating human rotavirus strain and uses African Green monkey kidney cells to produce the original viral seed stock from which the vaccine has been made.
Inclusion of rotavirus vaccine(s) in the infant vaccine schedule is being vigorously encouraged by medical groups such as the Canadian Paediatric Society and Canada's National Advisory Committee on Immunization who recommend that all babies be vaccinated against rotavirus. The vaccine is given orally in two or three doses, starting at 6 weeks of age and ending no later than 8 months. It is not recommended for children after age three.
In a recent Canada Communicable Disease Report, we are told that, "the number of seizures reported among vaccine recipients was consistently higher than that reported among placebo recipients in each time interval after immunization."
The current vaccine, RotaTeq, marketed by Merck Frosst Canada, is a second generation vaccine, developed after the first version, RotaShield produced and marketed by Wyeth-Ayerst Laboratories was pulled from the market because of reports of bowel obstruction developing within weeks of vaccination. The Vaccine Adverse Events Reporting System (VAERS) in the U.S revealed persistent reports of vomiting and diarrhea following receipt of rotavirus vaccine and a number of infant deaths.
Conclusions: "These observations, coupled with limited rotavirus disease burden, cost-effectiveness, and potential contact viral transmission concerns, raise serious questions regarding the use of RotaTeq in the US. Healthcare providers should diligently report adverse events following RotaTeq vaccination to VAERS..."('RotaTeq vaccine adverse events and policy considerations' by David A. Geier et al.)
A June 15, 2011 WebMD bulletin reports that a large Latin American study found that while "the risk appears to be small" and..."between 1 in 51,000 and 1 in 68,000 vaccinated babies given the rotavirus vaccine Rotarix, manufactured by GlaxoSmithKline, could be expected to develop intussusception, a condition in which part of the intestine slides into another part of the intestine, like parts of a telescope."
Rarely mentioned is the importance of breastfeeding as an effective preventive of a wide range of gastrointestinal diseases in infants while mitigating the severity of rotavirus disease. Research over many decades has shown that formula fed babies are much more susceptible to severe gastrointestinal illnesses.
Vaccines developed to prevent rotavirus are limited in their effectiveness, and cause a host of health problems. According to the aforementioned CDC report, "the vaccine demonstrated 49%-68% efficacy against any rotavirus diarrhea".
As with most other vaccine mitigated diseases, deaths occur almost exclusively in under developed countries, and are due to malnutrition, parasites, and co-infection with other diseases such as malaria and yellow fever.
The original rotavirus vaccine RotaShield, marketed by Lederle, was withdrawn after a year because of an association with a serious gastric condition intussusception in which the bowel folds in on itself causing a blockage. Intussusception can kill. Reports on VAERS (Vaccine Adverse Event Reporting System) for Lederle's RotaShield lists 124 reported cases of intussusception in one of which the patient died (1 in 124). The newer products, Merck's RotaTeq, which Paul Offit helped to develop and profitted from, and GSKs Rotarix are both associated with an elevated level of intussusception. Reports on VAERS (9 February 2015) for the Offit/Merck Rotateq vaccine introduced in 2006 list 1,068 cases of intussusception with 10 accompanying deaths (1 in 107) while Rotarix (introduced in 2008?) has 553 cases of intussusception and 11 deaths (a very disturbing rate of 1 in 50). It is not known how many doses of the respective vaccines this represents.
Intussusception is a symptom specifically associated with rotavirus vaccines. It should be borne in mind that these vaccines have seldom been administered separately from other vaccines, however reports of total outcomes on VAERS in which the patient died are alarmingly high:
A problem with exposure to multiple vaccines all at one time is that they increase the overall risk of death. Another problem is that the multiple shots make it difficult to figure out which vaccines are doing what. However, as a point of comparison there have been 425 deaths associated with rotavirus vaccines since 2006, compared with a mere 329 for MMR since 1989.
This LINK leads to a multiplicity of other sources of information about rotavirus vaccines.
Smallpox
Amidst recent growing concerns about bioterrorism, smallpox vaccination has resurfaced from the history books to become a topic of major importance. Inoculation with vaccinia virus is highly effective for the prevention of smallpox infection, but it is associated with several known side effects that range from mild and self-limited to severe and life-threatening.
The World Health Assembly declared that smallpox had been eradicated from the earth in 1980. The efficacy of the vaccine has not been evaluated in controlled studies, but epidemiologic data suggest that a high level of protection persists for up to 5 years after vaccination, with partial immunity persisting for 10 years or more. The vaccine will prevent infection or reduce the severity of illness if given within a few days following exposure to smallpox.
Smallpox vaccine is less safe than other vaccines routinely used today. The vaccine is associated with known adverse effects that range from mild to severe. Mild vaccine reactions include formation of satellite lesions, fever, muscle aches, regional lymphadenopathy, fatigue, headache, nausea, rashes, and soreness at the vaccination site.
In the 1960s, serious adverse events associated with smallpox vaccination in the United States included death (1 per million vaccinations), progressive vaccinia (1.5 per million vaccinations), eczema vaccinatum (39 per million vaccinations), postvaccinial encephalitis (12 per million vaccinations), and generalized vaccinia (241 per million vaccinations). Adverse events were approximately ten times more common among those vaccinated for the first time compared to revaccinees. Fatality rates were also four times higher for primary vaccinees compared to revaccinees.
The most common adverse event associated with smallpox vaccination is accidental infection with smallpox itself, occurring at a rate of 529 per million vaccinations in one study. [link is to summary; full text is pdf]
Less common, but certainly more horrific is progressive vaccinia (a.k.a. vaccinia necrosum, vaccinia gangrenosum). In common terms, it is spreading tissue death, the mechanism of which is gangrene. It is literally uncontrolled growth of the vaccine virus that spreads over the body and then to tissues and organs, ultimately leading to death.
Then there is eczema vaccinatum, a cutaneous dissemination of vaccine virus that usually occurs in persons with pre-existing skin disease. It is typically mild and self-limited, but it may be severe or fatal, especially in young children. Death is usually caused by extensive viral dissemination, fluid and electrolyte imbalance, and bacterial sepsis. Improvements in intensive care therapy during the 1960s likely contributed to the lowering of the fatality rate for eczema vaccinatum from 10% to 1% to 2%.
Encephalopathy, or swelling of the brain, is an adverse side effect of many different vaccines, and the smallpox vaccine is highest on that list. Post-vaccinial encephalitis is a rare adverse event that frequently leads to death, especially in infants and young children. Reported case fatality rates range from 9% to 40%. Ten to twenty-five percent of surviving patients have permanent neurologic conditions.
Vaccinia virus may be spread from person-to-person, which means that people who have close contact with recently vaccinated people may be exposed to the virus and may be at risk of developing complications.
Current event in Mexico leaves two babies dead, 13 in critical condition, 37 out of 52 injured
This is from Sanevax.org dated May 11, 2015:
The indigenous municipality of Simojovel, in the state of Chiapas, Mexico reported the death of two babies after the administration of vaccines against hepatitis B (HepB), tuberculosis (BCG), and rotavirus.
Within hours of receiving the vaccines, 37 babies out of a total of 52 vaccinated had adverse reactions; some began to convulse with the tragic result of two dead and 37 hospitalized, 13 of whom reported to be in critical condition. According to the Catholic organization Pueblo Creyente, the dead included a 30-day-old girl and a 28-day-old boy.
The Mexican Social Security Institute (IMSS) ordered the preventive suspension of the BCG (Tuberculosis), Rotavirus and Hepatitis B vaccine, after what they suspect were allergic reactions to the vaccines administered to the minors in Chiapas.
Although this news has been widely disseminated in the Spanish-language press, it has been virtually ignored by the English-language press.
(3) Serious complications of measles, whooping cough and influenza are reduced through the use of vitamins A and C. People don't die from these diseases. They die from complications of these diseases.
You will note in the first graph that the incidence of deaths due to measles had plummeted prior to 1961 when the vaccine was introduced. That is because mortality in measles cases occurs primarily among the population that suffers from malnutrition. Many measles deaths can be attributed to near starvation conditions. Even if there is an adequate amount of calories overall, protein deficiency is a common occurrence. South African Medical Journal Vol. 68 December 1985 "Factors associated with fatal cases of measles" A. Beckford, et al
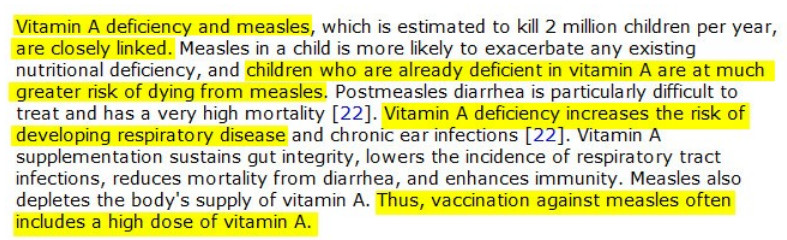
Vitamin A deficiency and measles, which is estimated to kill 2 million children per year, are closely linked. Vitamin A supplementation (see below) sustains gut integrity, lowers the incidence of respiratory tract infections, reduces mortality from diarrhea, and enhances immunity. Lack of this and other vitamins, plus deficiency of minerals like zinc and iron, as well as inadequate access to clean drinking water accounted for the high levels of deaths due to measles and other infectious diseases. Other factors include parasite infection, co-infection with diarrheal diseases, tetanus, yellow fever and malaria.
According to the USA National Institutes of Health "Treatment with vitamin A reduces morbidity and mortality in measles, and all children with severe measles should be given vitamin A supplements, whether or not they are thought to have a nutritional deficiency."
Clive E. West, PhD, DSc, "Vitamin A and Measles", Nutrition Reviews, vol. 58, no. 2, February 2000, p. S46. -
Vitamin A deficiency affects the severity of illness and the rate of deaths associated with measles, and it is known to induce severe measles-related complications in children, delaying recovery and promoting xerophthalmia, corneal ulcer, and blindness. Acute measles precipitates vitamin A deficiency by depleting vitamin A stores and increasing its utilization, leading to more severe ocular injury. Vitamin A supplementation given to children with measles has been associated with better outcomes. US CDC
Vitamin A stops the measles virus from rapidly multiplying inside cells by up-regulating the innate immune system in uninfected cells which helps to prevent the virus from infecting new cells. It is well known today that a low vitamin A level correlates with increased morbidity and mortality. Vitamin A is a well-proven intervention for reduction of mortality, concomitant infections, and hospital stay. Wafaie W. Fawzi, MD; Thomas C. Chalmers, MD; M. Guillermo Herrera, MD; and Frederick Mosteller, PhD, “Vitamin A Supplementation and Child Mortality: A Meta-Analysis,” Journal of the American Medical Association, February 17, 1993, p. 901.
The efficiency of the cellular immune system is tied to the intake of dietary nutrients, including vitamin A, vitamin C, zinc, selenium, and protein rich in vitamin B. Poor nutrition leads to impaired cellular immune responses, which results in worse outcomes after measles infection or exposure. D. N. McMurray, “Cell-Mediated Immunity in Nutritional Deficiency,” Progress in Food & Nutrition Science, 1984, p. 193.
Experiments done in the 1940s showed that vitamin C was effective against measles, especially when used in higher doses.
"During an epidemic [of measles] vitamin C was used prophylactically and all those who received as much as 1000 mg. every six hours, by vein or muscle, were protected from the virus. Given by mouth, 1000 mg. in fruit juice every two hours was not protective unless it was given around the clock. It was further found that 1000 mg. by mouth, four to six times each day, would modify the attack; with the appearance of Koplik’s spots and fever, if the administration was increased to 12 doses each 24 hours, all signs and symptoms would disappear in 48 hours." Fred R. Klenner, MD, “The Treatment of Poliomyelitis and Other Virus Diseases with Vitamin C,” Southern Medicine & Surgery, July 1949.
(4) The option of informed consent is never even presented to parents in the context of the decision to vaccinate their children
At the 1982 Forum of the American Academy of Pediatrics (AAP), the adoption of the following resolution was urged by a concerned member:
"The AAP [will] make available in clear, concise language information which a reasonable parent would want to know about the benefits and risks of routine immunizations, the risks of vaccine preventable diseases and the management of common adverse reactions to immunizations." Resolution presented to American Academy of Pediatrics, 1982 Forum.
After careful deliberation, the resolution was rejected. Therefore, parents continue to not be told of the risks of vaccination. It remains rejected to this very day.
Informed consent prior to any medical intervention is a basic human right. By definition, informed consent gives you the right to analyze the risks and benefits of the proposed medical intervention then refuse (opt out) of having the procedure performed if the risks outweigh the benefits for you as an individual. The problem is many people seem to have forgotten vaccines are a medical intervention.
Patients or legal guardians thereof have a moral right to freedom of choice when it comes to medical procedures. We do recognize the right of the state to enforce life saving procedures for minor children and mentally incapacitated individuals where the proof of necessity is overwhelming. The state must, in turn, recognize the right of individuals or their legal guardians to choose various options where the basis of choice is between reasonably equal alternatives. It can be proven that the argument as to whether or not the risks of injury or death from vaccines is as weighty as the possible benefit from receiving the vaccines.
The vaccination programs as now conducted are best viewed as mass experimentation upon humans that is improperly conducted. The code of conduct gold standard is the Nuremberg code which was formed to prosecute and punish war criminals following World War 2. It includes such principles as informed consent and absence of coercion; properly formulated scientific experimentation; and beneficence towards experiment participants. This code applies to medical experiments performed upon human subjects. It is logically shown that the vaccination programs carried out in modern times are, in fact, experiments by every possible definition, not efforts based upon settled science.
(5) "Herd immunity" is not what you've been told it is
:Herd immunity" has nothing to do with vaccines. It is widely misunderstood because its history and meaning have been corrupted by the pharmaceutical industry.
Measles
From Vaccine Choice Canada:
The term, 'herd immunity', was coined by researcher, A. W. Hedrich, after he had studied the epidemiology of measles in USA between 1900-1931. His study published in the May, 1933 American Journal of Epidemiology concluded that when 68% of children younger than 15 years old had become immune to measles via infection, measles epidemics ceased. For several reasons, this natural, pre-vaccine herd immunity differed greatly from today's vaccine 'herd immunity'.
When immunity was derived from natural infection, a much smaller proportion of the population needed to become immune to show the herd effect; compare the 68% measles immunity required for natural herd immunity to the very high percentages of vaccine uptake deemed necessary for measles vaccine 'herd immunity'. In his Vaccine Safety Manual, Neil Z. Miller cites research which concluded increasing vaccine uptake necessary for 'herd immunity' ranging from '70 to 80 percent of two year-olds in inner cities' in 1991 to 'close to 100 percent coverage'...with a vaccine that is 90 to 98 percent effective.' in 1997. Miller notes that, "When the measles vaccine was introduced in 1963, officials were confident that they could eradicate the disease by 1967."
By examining case numbers reported by the California Department of Public Health and current and historical case data captured by the HealthMap disease surveillance system, the researchers — led by Maimuna Majumder, MPH, and John Brownstein, PhD, of Boston Children's Informatics Program — estimate that the measles vaccination rate among the case clusters in California, Arizona and Illinois is between 50 and 86 percent, far below the 96 to 99 percent believed by pro-vaccine advocates to be necessary to create a herd immunity effect.
The measles vaccine failure rate is much higher than we are lead to believe. In a 2012 paper titled "The Deadly Impossibility of Herd Immunity Through Vaccination" Dr. Russell Blaylock explains it this way.
"That vaccine-induced herd immunity is mostly myth can be proven quite simply. When I was in medical school, we were taught that all of the childhood vaccines lasted a lifetime. This thinking existed for over 70 years. It was not until relatively recently that it was discovered that most of these vaccines lost their effectiveness 2 to 10 years after being given. What this means is that at least half the population, that is the [later] baby boomers, have had no vaccine-induced immunity against any of these diseases for which they had been vaccinated very early in life. In essence, at least 50% or more of the population was unprotected for decades.
If we listen to present-day wisdom, we are all at risk of resurgent massive epidemics should the vaccination rate fall below 95%. Yet, we have all lived for at least 30 to 40 years with 50% or less of the population having vaccine protection. That is, herd immunity has not existed in this country for many decades and no resurgent epidemics have occurred. Vaccine-induced herd immunity is a lie used to frighten doctors, public-health officials, other medical personnel, and the public into accepting vaccinations.
When we examine the scientific literature, we find that for many of the vaccines protective immunity was 30 to 40%, meaning that 70% to 60% of the public has been without vaccine protection. Again, this would mean that with a 30% to 40% vaccine-effectiveness rate combined with the fact that most people lost their immune protection within 2 to 10 year of being vaccinated, most of us were without the magical 95% number needed for herd immunity. This is why vaccine defenders insist the vaccines have 95% effectiveness rates."
The fact is that 86% of the people who contracted measles at Disneyland were vaccinated. Yet, they came down with measles. That is because the vaccines are not as effective as claimed. This information comes from California Healthcare Foundation.
Pertussis
"Our unvaccinated and under-vaccinated population did not appear to contribute significantly to the increased rate of clinical pertussis. Surprisingly, the highest incidence of disease was among previously vaccinated children in the eight to twelve year age group." In a statement from the US National Institutes of Health titled "Unexpectedly limited durability of immunity following acellular pertussis vaccination in preadolescents in a North American outbreak".
Again, from Vaccine Choice Canada:
Disease-conferred immunity usually lasted a lifetime. As each new generation of children contracted the infection, the immunity of those previously infected was renewed due to their continual cyclical re-exposure to the disease; except for newly-infected children and the few individuals who'd never had the disease or been exposed to it, the herd immunity of the entire population was maintained at all times.
Vaccine "herd immunity" is hit-and-miss; outbreaks of disease sometimes erupt in those who follow recommended vaccine schedules. If they do actually "immunize", vaccines provide only short-term immunity so, in an attempt to maintain "herd immunity", health authorities hold "cattle drives" to round up older members of the "herd" for administration of booster shots. And on it goes, to the point that, now, it's recommended we accept cradle-to-grave shots of vaccine against pertussis, a disease which still persists after more than sixty years of widespread use of the vaccine.
In the pre-vaccine era, newborns could receive antibodies against infectious diseases from their mothers who had themselves been infected as children and re-exposed to the diseases later in life. Today's babies born to mothers who were vaccinated and never exposed to these diseases do not receive these antibodies. In direct contrast to fear mongering disease "facts" and "herd immunity" theories related by Public Health, most of today's babies are more vulnerable than babies of the pre-vaccine era.
Dr. Russell Blaylock puts it succinctly.
"One of the grand lies of the vaccine program is the concept of 'herd immunity'. In fact, vaccines for most Americans declined to non-protective levels within 5 to 10 years of the vaccines. This means that for the vast majority of Americans, as well as others in the developed world, herd immunity doesn't exist and hasn't for over 60 years."
(6) The increase in the number of vaccines, and the early age at which they are routinely administered, causes more and more disorders.
Babies and very young children are now bombarded with vaccines from the moment they are born. Part of the problem is the fact that from the original 8 recommended childhood vaccines, now a child would receive 49 doses of 14 medications by age 6. Extending the time period to include the teenage years brings the total to 69 doses of 16 vaccines by age 18.
A confidential study conducted by Connaught Laboratories, a vaccine manufacturer, indicated that "a fifty-fold under-reporting of adverse events" is likely. According to David Kessler, former commissioner of the FDA, "only about one percent of serious events [adverse drug reactions] are reported."
Thus, the increased mortality and hospitalization suffered by children as a direct result of the aggressive vaccination schedule, with as many as 9 vaccines given in one day, is a huge number of children. If, according to the study's report above, only 1 to 2 out of 100 adverse events is reported, then the numbers reported by VAERS need to be multiplied by 50 to 100!
From the journal HUMAN & EXPERIMENTAL TOXICOLOGY
The deaths of children from multiple vaccine doses can only be called carnage. This study demonstrates that giving 5-8 doses instead of 1-4 doses at a time has resulted in an extra 51,750 to 103,500 child deaths in the last 20 years.
Studies have not been conducted to determine the safety (or efficacy) of administering multiple vaccine doses in a variety of combinations as recommended by CDC guidelines. Findings show a positive correlation between the number of vaccine doses administered and the percentage of hospitalizations and deaths reported to VAERS. In addition, younger infants were significantly more likely than older infants to be hospitalized or die after receiving vaccines. Since vaccines are administered to millions of infants every year, it is imperative that health authorities have scientific data from synergistic toxicity studies on all combinations of vaccines that infants are likely to receive; universal vaccine recommendations must be supported by such studies.
**footnotes in this section refer to this CDC report:
The people who suffer adverse reactions to vaccines often are infants and children; 45% of reports to VAERS concern children age six and under.44 The problems incurred as a result of vaccination go far beyond sore arms and transitory fever. Adverse events such as anaphylaxis, Guillain-Barre syndrome, brachial neuritis, thrombocytopenia, poliomyelitis (caused by the oral polio vaccine, no longer used in the US), acute encephalopathy, and hypotonic/hyporesponsive episodes have been linked to vaccines.45-48
Serious adverse events [
Overall, 14.2% of all reports received in VAERS during 1991--2001 described serious adverse events (10 - pdf) (Table 9). During 1991--2001, reports of deaths ranged from 1.4%--2.3%, and reports of life-threatening illness ranged from 1.4%--2.8% of all adverse event reports. During the previous 3 years when distribution of vaccines reached the highest level, the annual percentage of reports of death was stable, approximately 1.5% of all adverse event reports.
CDC's own data shows SIDS linked to vaccinations 51% of the time
A clinical research team follows up on all deaths reported to VAERS. The majority of these deaths were ultimately classified as sudden infant death syndrome (SIDS). Analysis of the age distribution and seasonality of infant deaths reported to VAERS indicated that they matched the age distribution and seasonality of SIDS; both peaked at aged 2--4 months and during the winter (15). The decrease in deaths reported to VAERS since 1992--1993 parallels the overall decrease in SIDS in the U.S. population since the implementation of the Back to Sleep campaign (15). Carefully controlled epidemiologic studies consistently have not found any association between SIDS and vaccines (16, 17, 18, 19). FDA and the Institute of Medicine (IOM) reviewed 206 deaths reported to VAERS during 1990--1991. Only one death was believed to have resulted from a vaccine. The patient was a woman aged 28 years who died from Guillain-Barré syndrome after tetanus vaccination (20). IOM concluded that the majority of deaths reported to VAERS are temporally but not causally related to vaccination (20). A similar conclusion was reached regarding neonatal deaths temporally reported to VAERS in association with hepatitis B vaccination (21).
Some research also has suggested that sudden infant death syndrome (SIDS) is associated with vaccinations.49-51 A study by FDA researchers of reports to VAERS from 1991 to 1994 found that most of the reported deaths were attributed to SIDS. The researchers concluded, however, that "the peak age of deaths at ages one to three months could be expected on the basis of prior studies showing that sudden infant death syndrome deaths peak at that age."52 Similarly, the CDC's study of VAERS data from 1991 to 2001 found that the majority of deaths reported were ultimately designated as SIDS. This report also concluded that the age distribution and seasonality of the infant deaths reported to VAERS matched those of SIDS. The CDC cites other research discounting an association between vaccinations and untimely deaths of infants.53,54 Critics have noted, however, that a comparison with the background rate of SIDS among vaccinated populations, rather than comparable unvaccinated groups, is not meaningful.55 [END OF LINKED REPORT]
Here is just one anecdotal report. It will break your heart.
The actual evidence from the CDC's scientific and clinical literature produced by these very agencies contradicts their own vaccine policies.
This is exactly what has happened with the publication of a new study in the Journal of Pediatrics titled ,"Adverse Events following Haemophilus influenzae Type b Vaccines in the Vaccine Adverse Event Reporting System, 1990-2013," wherein CDC and FDA researchers identify 749 deaths linked to the administration of the Hib vaccine, 51% of which were "sudden-infant-death" linked to the administration of Hib vaccine.
This is madness. Absolute insanity. Presently, the CDC recommends 4 doses of the HiB vaccine at the following ages: 2 months, 4 months, 6 months, 12 months through 15 months.
Consider also that VAERS is a passive surveillance system, which suffers from profound underreporting. According to the VAERS site's own disclaimer:
"Underreporting is one of the main limitations of passive surveillance systems, including VAERS. The term, underreporting refers to the fact that VAERS receives reports for only a small fraction of actual adverse events. The degree of underreporting varies widely. As an example, a great many of the millions of vaccinations administered each year by injection cause soreness, but relatively few of these episodes lead to a VAERS report."
According to Barbara Loe Fisher, founder of the National Vaccination Information Center, underreporting may result in overlooking 99% or higher of all vaccine associated injuries.
It just goes on and on. The links between various vaccines and Autism Spectrum Disorders are too numerous to count, both in the scientific literature and in popular anecdotal accounts. The correlation between the numerical rise in these disorders and the increase in vaccinations scheduled for toddlers through teens is blatantly apparent.
Autistic conditions can result from encephalopathy following vaccination. The US Health Resources and Services Administration (HRSA) confirmed to CBS News that of 1,322 cases of vaccine injury compensation settled out of court by the US Government in secret settlements:
"We have compensated cases in which children exhibited an encephalopathy, or general brain disease. Encephalopathy may be accompanied by a medical progression of an array of symptoms including autistic behavior, autism, or seizures."
[PDF Download — Text of email from US HRSA to Sharyl Attkisson of CBS News]
Autistic conditions can result from acute disseminated encephalomyelitis (ADEM) following MMR vaccination as held by the US Federal Court in the case of Bailey Banks. In his conclusion, US Federal Court Special Master Abell ruled that Petitioners had proven that the MMR had directly caused a brain inflammation illness called acute disseminated encephalomyelitis (ADEM) which, in turn, had caused the autism spectrum disorder PDD-NOS in the child.
"The Court found that Bailey's ADEM was both caused-in-fact and proximately caused by his vaccination. It is well-understood that the vaccination at issue can cause ADEM, and the Court found, based upon a full reading and hearing of the pertinent facts in this case, that it did actually cause the ADEM. Furthermore, Bailey's ADEM was severe enough to cause lasting, residual damage, and retarded his developmental progress, which fits under the generalized heading of Pervasive Developmental Delay, or PDD [an autism spectrum disorder]. The Court found that Bailey would not have suffered this delay but for the administration of the MMR vaccine, and that this chain of causation was....a proximate sequence of cause and effect leading inexorably from vaccination to Pervasive Developmental Delay." LINK
In 2002, the Chief Master of the U.S. Court of Federal Claims created the Omnibus Autism Proceeding to adjudicate petitions filed with VICP alleging autism or autism spectrum disorder from either the MMR vaccine or thimerisol-containing vaccines, or from both. Anticipating large numbers of claims, the Court allowed the filing of "shortform" petitions, but without medical records. As a result, a very small number of the pending 5,000 claims have medical records, making it impossible for us to review and compare commonalities, patterns, or any general trends among all of the petitioners. Over time, we may learn more about patterns of pre-existing conditions and the role vaccines play, if any, in their progression. As we have done in the past, the VICP medical staff will look at the court findings and any new scientific information, and may publish scientific articles as appropriate.
(7) Natural immunity is better than the vaccine induced kind
This whole, long treatise I have put together revolves around the topic of immunity. At the heart of the issue is the human body's immune system. It has two branches.
-
The humoral system (or Th2 function) produces antibodies in the blood that recognize foreign antigens (invaders) in the body.
-
The other branch is the cellular or cell-mediated immune system (or Th1 function), which primarily destroys, digests and expels foreign antigens out of the body through the activity of its cells found in the thymus, tonsils, adenoids, spleen, lymph nodes and lymph system throughout the body.
This process of destroying, digesting and discharging foreign antigens from the body is known as "the acute inflammatory response" and is often accompanied by the classic signs of inflammation: fever, pain, malaise and discharge of mucus, pus, skin rash or diarrhea. The two systems should balance each other to work properly. The problem is that over-stimulating antibody production can suppress the acute inflammatory response of the cellular immune system!
Vaccines are intended to supercharge the humoral system. Not only do they contain viruses, bacteria and other antibody triggers, but they also contain foreign substances like aluminum, mercury and other stimulants. Here is where we run into trouble.
"A vaccination consists of introducing a disease agent or disease antigen into an individual's body without causing the disease. If the disease agent provoked the whole immune system into action it would cause all the symptoms of the disease! The symptoms of a disease are primarily the symptoms (fever, pain, malaise, loss of function) of the acute inflammatory response to the disease.
"So the trick of a vaccination is to stimulate the immune system just enough so that it makes antibodies and remembers the disease antigen, but not so much that it provokes an acute inflammatory response by the cellular immune system and makes us sick with the disease we're trying to prevent!" PHILIP F. INCAO, M.D.
The two two systems could be compared to two aspects of the eating process. One could be the tasting and recognizing of food (humoral system) and the other would be digesting and eliminating waste (cellular system). But, just as tasting too much food can ruin the appetite, too much repeated stimulation of the cellular branch of the immune system by an antigen will inhibit and suppress the digesting and eliminating function of the cellular immune system. In other words, over stimulating antibody production can suppress the acute inflammatory response of the cellular immune system!
In plain terms, there are two types of inflammation. Stimulation of the humoral system by antigens found in vaccines produces autoimmune inflammations like allergies. This prevents the body from experiencing acute discharging inflammations like fever, pain and malaise. The more a person has of one, the less he or she will have of the other. It is not difficult to see then why the repeated use of vaccinations would tend to shift the functional balance of the immune system toward the antibody-producing side (Th2) and away from the acute inflammatory discharging side (the cell-mediated side or Th1).
Speaking of fever, it is important to realize that fever is the body's way of fighting pathogens. When a child has measles and runs a fever, it is counter productive to give him or her fever reducers. There is actually a "fever phobia" exhibited by parents in many cases.
"Parents are telling us that they're worried that fever can cause brain damage or even death in their children," said Dr. Michael Crocetti, an assistant professor of pediatrics at Johns Hopkins and lead author of the 2001 study. "I've been doing this for a long time, and it seems to me that even though I do a tremendous amount of education about fever, its role in illness, its benefit in illness, it doesn't seem to be something they keep hold of from visit to visit."
Dr. Janet Serwint, another author of the study and a professor of pediatrics at Johns Hopkins, agreed. "I personally think there should be much more education about this at well visits," she told me, adding that parents need to understand "the helpfulness of fever — how fever actually is a well-orchestrated healthy response of our body." (LINK)
Fever can indeed be scary, and any fever in an infant younger than 3 months is cause for major concern because of the risk of serious bacterial infections. But in general, in older children who do not look very distressed, fever is positive evidence of an active immune system, revved up and helping an array of immunological processes work more effectively.
This brings us to the "hygiene hypothesis" that is now coming into favor among many medical scientists. In September 2011, German researchers carrying out a longitudinal study surveyed a total of 8000 unvaccinated children from the ages of 0 —19. As with the New Zealand study, researchers collected their data by conducting a survey using questionnaires. Results showed that vaccinated children were up to five times more likely to suffer from a variety of diseases and disorders than unvaccinated children.
Compared to unvaccinated children, vaccinated children were more likely to suffer from asthma, eczema, ear infections, hyperactivity and many other chronic conditions. Furthermore, the study identified that there was a ten-fold increase in the incidence of tonsillitis in the children who were vaccinated, and a total lack tonsillectomy operations among the children who were unvaccinated. (LINK)
Also, scientists have known since the earliest days of childhood disease vaccines that antibodies aren't even necessary to fight off measles. One of the most disconcerting discoveries in clinical medicine was the finding that children with congenital agamma-globulinaemia, who could make no antibody and had only insignificant traces of immunoglobulin in circulation, contracted measles in normal fashion, showed the usual sequence of symptoms and signs, and were subsequently immune. No measles antibody was detectable in their serum [the water part of blood minus clotting factors and cells].
Vaccine scientists and public health officials have measured "immunity" solely focusing on antibodies. Antibody production does occur in natural infection but it is the last thing that happens and not a necessary part of recovery or long-term immunity. It is known that the immune system responds with more than just antibodies, yet because markers of cell-mediated immunity are elusive, antibodies have become the measure of whether or not a person is immune.
Antigen: (antibody generator): An antigen is any substance that causes your immune system to produce antibodies against it. An antigen may be a foreign substance from the environment, such as chemicals, bacteria, viruses, or pollen. An antigen may also be formed inside the body, as with bacterial toxins or tissue cells.
Antibody: An antibody (AB), also known as an immunoglobulin (Ig), is a large Y-shape protein produced by plasma cells that is used by the immune system to identify and neutralize foreign objects such as bacteria and viruses. The antibody recognizes a unique part of the foreign target, called an antigen.
True immunity no longer goes from mother to baby through placenta
Mothers transmit all sorts of protective immune globulins to their babies naturally via the placenta, and these last for several months following birth. They also pass general and specific immunity through their milk. A mother who has had natural measles yields protection to the baby against measles for about 12 to 15 months while breastfeeding. Mothers who were vaccinated transmit a shorter duration of protection to their babies. In the era of vaccination, babies are now susceptible to measles at a much earlier age. Consequently, the medical community now calls for babies to have their first MMR vaccine at a much earlier age, usually six months.
The mothers might not even have immunity to pass along, if they haven't kept up on booster shots. Since a huge percentage of adults are themselves no longer immune due to the vaccines' short lives, they can't possibly pass along protection to a baby through placental fluid or breast milk.
Lifetime immunity
Acquiring innocuous childhood diseases such as chicken pox, measles, mumps and rubella can help to build immunity and give your child lifetime protection against these diseases. Lifetime immunity is important since these diseases can have serious negative effects if one is infected as an adult.
When infectious diseases of childhood are not mismanaged by the administration of antibiotics, or by suppressing fever, the diseases prime and mature the immune system, and also represent developmental milestones. Having measles not only results in life-long specific immunity to measles, but also in life-long non-specific immunity to degenerative diseases of bone and cartilage, sebaceous skin diseases, immunoreactive diseases and certain tumors as demonstrated by Ronne (1985). Having mumps protects against ovarian cancer (West 1969).
"VACCINATIONS are usually effective in preventing an individual from manifesting a particular illness, but they DO NOT IMPROVE the overall STRENGTH or HEALTH of the individual nor of the immune system. Instead, VACCINATIONS MODIFY the REACTIVITY of the IMMUNE SYSTEM, decreasing acute discharging inflammatory reactions and INCREASING the TENDENCY to CHRONIC ALLERGIC and AUTO-IMMUNE REACTIONS." INCAO [capitalization his]
(8) Additives in manufactured vaccines are highly toxic, and we inject them directly into our bloodstream.
Mercury is famous for causing brain damage, and it used to be in most of our common vaccines in the form of Thimerosal (a.k.a. Thiomersal) preservative. Experts have for some time said that it is partly responsible for Autism Spectrum Disorders, including ADHD. It has now been removed from most of them. This would seem to be hopeful news for the parents of babies but, no, the news is still grim. It is still in flu vaccines and, unfortunately, they are recommended both for pregnant mothers and for six month old infants.
Even the vaccines from which the mercury has been removed may still contain "trace amounts" of the substance, which the CDC defines as being 3 micrograms of mercury, 150 times higher than what the EPA considers "safe" for drinking water (for adults). And, the amounts of mercury that were in vaccines prior to their removal were much higher than the percentages still in use. A lot of people were affected by mercury before even the most meager efforts were made to remove it from vaccines.
It doesn't take much to affect fetuses and infants where the brain is growing and developing by leaps and bounds. And, when it was removed, highly toxic aluminum compounds replaced them. These chemicals were added for two purposes. First they were used as preservatives, to keep bacteria from growing in the vaccines. Remember having cuts and scrapes painted with mercurochrome antiseptic as a kid? That redd-ish stuff with the metalic overtones? It was banned for sale and use in the US in 1998 due to its mercury content.
More on the second purpose, shortly.
Mercury is still in flu shots!
 From 1999 to 2002 most mercury laced vaccines were phased out. Did autism rates decline? No they did not. That is because aluminum was added to those vaccines to take mercury's place. During the so-called phase out, authorities actually added mercury-laced flu shots to the list of all vaccines urged for babies aged 6 to 23 months old. Soon after they also added pregnant mothers in their first trimester to the list of people who were encouraged to receive the mercury-laced flu vaccines.
From 1999 to 2002 most mercury laced vaccines were phased out. Did autism rates decline? No they did not. That is because aluminum was added to those vaccines to take mercury's place. During the so-called phase out, authorities actually added mercury-laced flu shots to the list of all vaccines urged for babies aged 6 to 23 months old. Soon after they also added pregnant mothers in their first trimester to the list of people who were encouraged to receive the mercury-laced flu vaccines.
Depending on the vaccines administered, at six months of age, infants today born to mothers who received flu vaccine during pregnancy could receive up to 71 mcg of ethyl mercury compared to 187.5 mcg prior to efforts to decrease the amount of thimerosal in infant vaccines. Additionally, the new CDC guidelines recommend that all children from 2 to 5 years of age receive an annual influenza vaccine. As a result, the total amount of Thimerosal given to children under 5 years of age is almost what it was prior to 2000.
Manufacturers began voluntarily removing Thimerosal from pediatric vaccines around 2000. It is assumed that most pediatric vaccines containing Thimerosal were "off the shelves" by 2003. (No vaccines were recalled.) Even so, most infants are still routinely given Thimerosal-containing influenza vaccine even though there are Thimerosal-free vaccines. Infants receiving a Thimerosal-containing influenza vaccine are dosed at 6 months with 12.5 mcg of ethyl mercury and at 7 months with an additional 12.5 mcg. Adult Thimerosal-containing vaccines contain roughly 25mcg.
In 2001 the European Agency for the Evaluation of Medicinal Products advised doctors to use only vaccines without Thimerosal for toddlers and infants, who are thought to be more likely to suffer harm from exposure to mercury. This followed a 1999 announcement by the U.S. Public Health Service and the American Academy of Pediatrics (AAP) that Thiomersal should be reduced or eliminated in vaccines as a precaution.
A study by the American Institute of Medicine concluded that a link between Thiomersal in vaccines and neuro- developmental disorders "including autism" was 'biologically plausible'. In a related U.S. study, researchers found a 'statistically significant' association between Thiomersal in vaccines and children with problems such as attention deficit disorder and speech and language learning delays. LINK
Aluminum and other adjuvants
Additives are put into vaccines for a variety of purposes. In the early days of vaccines, live viruses were injected in patients in the hopes that the antibodies marshaled by the subject's immune system would create immunity to the disease. Not long thereafter, scientists started tinkering with additives to see if the vaccines could be made more effective.
One of the first adjuvants ever used was aluminum, an element known for its neurotoxicity. It's sobering to realize that when the aluminum adjuvant was first approved for use in vaccines, some 90 years ago, it was approved because of efficacy, tricking the immune system into thinking it was under attack. It was never actually tested for safety. Even the total allowable limit was based on efficacy data, not safety data. They just assumed it was safe.
Aluminum is a heavy metal with known neurotoxic effects on human and animal nervous systems. It can be found in these and other childhood vaccines — DTaP, Pediarix (DTaP-Hepatitis B-Polio combination), Pentacel (DTaP-HIB-Polio combination), Hepatitis A, Hepatitis B, Haemophilus influenzae B (HIB), Human Papilloma Virus (HPV), and Pneumococcal vaccines.
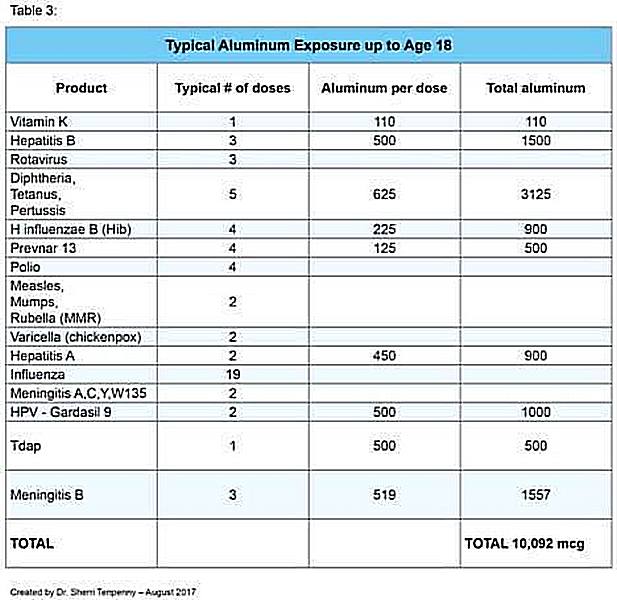
Aluminum is added to vaccines as an adjuvant so vaccines will produce a stronger antibody response in the misguided belief that this will make vaccines more protective. It is this role as an adjuvant that may reveal to us the most significant relationship between aluminum in vaccines and the damage it imparts on the long term health of our children's nervous and immune systems.
Furthermore, a growing number of studies have linked the use of aluminum adjuvants to serious autoimmune outcomes in humans. That concerns about aluminum adjuvant safety are indeed warranted is evident from the summary conclusions of the Aluminum in Vaccines workshop held in Puerto Rico in 2000 [Eickhoff, T.C.; Myers, M. Workshop summary. Aluminum in vaccines. Vaccine. 2002, 20 Suppl 3, S1-4.
"The literature demonstrates clearly negative impacts of aluminum on the nervous system across the age span. In adults, aluminum exposure can lead to apparently age-related neurological deficits resembling Alzheimer's and has been linked to this disease and to the Guamanian variant, ALS-PDC. Similar outcomes have been found in animal models. In addition, injection of aluminum adjuvants in an attempt to model Gulf War syndrome and associated neurological deficits leads to an ALS phenotype in young male mice. In young children, a highly significant correlation exists between the number of pediatric aluminum-adjuvanted vaccines administered and the rate of autism spectrum disorders. Many of the features of aluminum-induced neurotoxicity may arise, in part, from autoimmune reactions, as part of the ASIA syndrome." [ From the US National Library of Medicine National Institutes of Health ] https://pubmed.ncbi.nlm.nih.gov/15479434/
Early scientists also discovered that live viruses could sicken and even kill the patients they were intended to benefit. So, they tried killing viruses with various methods and injecting the killed viruses. One of the ways they settled on was the use of formaldehyde, also commonly used as embalming fluid. It did kill the viruses, and some success was met with the use of those inactivated viruses. Then too, there were some profound failures.
Among those failures was the first killed measles virus that was tried out in the 1960s, which was treated with formaldehyde. Early in that decade, measles was already at an 18 year low, so when the vaccine was introduced, it was credited with reducing the incidence of measles. That was an illusion, when the real reason was the natural dynamics of the disease. A curious phenomenon was also taking place. There were outbreaks and epidemics even in 100% vaccinated populations. Serious reactions including deaths were reported with increasing frequency.
It is less well known to the general public that vaccinated children started developing an especially vicious form of measles, due to the altered host immune response caused by the deleterious effect of the measles vaccines. It resisted all orthodox treatment and carried a high mortality rate. It has become known as atypical measles (AMS). The new atypical measles occurring in the vaccinated was characterized by high fever, unusual rash and pneumonia, often with history of vaccination with killed measles vaccine.
Adjuvants are substances that cause the humoral immune system to kick in with a strong reaction to these antigens. They promote strong inflammatory responses. As was mentioned earlier in the section on humoral versus cellular immune systems, frequent, strong stimulation of the humoral system does two things. It creates auto immune disorders and it partially disables the natural immune system.
For the most complete scientific text on adjuvants currently available, read Vaccine adjuvants: Current state and future trends in the journal Immunology & Cell Biology.
The CDC claims that Thimerosal is a relatively harmless form of mercury known as ethylmercury, which is rather quickly excreted from the human body. "Ethylmercury is formed when the body breaks down thimerosal. The body uses ethylmercury differently than methylmercury; ethylmercury is broken down and clears out of the blood more quickly. Low-level ethylmercury exposures from vaccines are very different from long-term methylmercury exposures, since the ethylmercury does not stay in the body."
This is why we can not trust the CDC! They lie through their teeth. The human body breaks down ethylmercury, alright. It converts it into methylmercury, which bioaccumulates in our tissues.
Either way, mercury or aluminum, we're still talking major neurotoxicity. In a study published in the Journal of the American Medical Association on May 29, 1997 called "Aluminum Neurotoxicity in Preterm Infants Receiving Intravenous-Feeding Solutions" the authors concluded the following:
For all 157 infants without neuromotor impairment, increasing aluminum exposure was associated with a reduction in the Mental Development Index (P = 0.03), with an adjusted loss of one point per day of intravenous feeding for infants receiving the standard solutions [containing aluminum]. CONCLUSION: in preterm infants, prolonged intravenous feeding with solutions containing aluminum is associated with impaired neurologic development.
So, let's just inject it into their bloodstreams so it goes right into their brains.
Documents obtained through the Freedom of Information Act show that Phase 1 of the CDC Thimerosal VSD Study found that there was increased risk of developing ADHD with cumulative exposure to thimerosal containing vaccines. Further, the lead author of the Thimerosal VSD Study indicated that the correlation in the Phase 1 results between increased neurological disorders and the vaccines could be found for aluminum in the vaccines as well as for mercury in the vaccines. In a different study reviewing the VSD data, "consistent significantly increased rate ratios" were observed for neurodevelopmental disorders including attention deficit disorder with mercury exposure from thimerosal containing vaccines. Although these findings were not included in the final publication of the Thimerosal VSD study, they warrant further research into whether vaccines contribute to ADHD.
Dr. Kenneth Bock states in his groundbreaking book Healing the New Epidemics that "ADHD is basically just the mildest form of symptom that is found on the autism spectrum. Both disorders, he contends are similar neurological manifestations of a wide variety of related problems. These include toxicity, bowel dysbiosis and allergic reactions."
Rates of attention-deficit/hyperactivity disorder, or ADHD, have crept upward over the past few years. Parents are now reporting that almost one out of 10 children and teens in the United States have been diagnosed with the condition at some point. The Centers for Disease Control and Prevention (CDC) conducted a nationwide survey of over 73,000 children's parents between April 2007 and July 2008. The results of this survey were compared to a similar survey conducted in 2003.
(9) The risk/benefit analysis is skewed
It is commonly assumed that the benefits of vaccines outweigh the risks. At some point in time that may have been true, but not since the 1980s, which is why vaccine manufacturers got immunity from law suits and criminal prosecution in 1986. Starting at that point in time, there is ample evidence that the increased number of recommended vaccines is linked to corresponding increases in childhood health conditions.
Do the benefits outweigh the risks of the current US vaccine schedule? To answer that question, we turn to a study done by smartvax.com.
We undertook a theoretical analysis to calculate the risk from diseases to an unvaccinated child in the first 5 years of life, and then compare that to the risk of vaccine-injury in the first 5 years of life if that child is vaccinated per the USA schedule. To make a valid comparison of disease risks to the unvaccinated child, we sought to calculate risk of injury from disease in two cases: 1) the risk in a highly vaccinated population and 2) the risk in a population with low vaccination. Where there is current evidence in the USA of herd immunity for a disease, this effect is considered in the highly vaccinated case (see A SmartVax Discussion on Herd Immunity). To perform the analysis, we made several assumptions about how to calculate risk (see Assumptions for Weigh The Risks Analysis) including a decision to focus on only four of the childhood chronic health conditions that may be vaccine-induced: Asthma, Autism, ADHD, and Allergies.
Importantly, this "Weigh The Risks" analysis found that the number of children affected just by asthma vaccine-injuries far greater than the number of children who would be affected by disease-injury or death today even in the worst-case disease scenario (in which herd immunity was not maintained):
[thanks to smartvax.com for the above text and graphic]
National Vaccine Information Center: "It is estimated that only between 1 and 10 percent of all adverse health outcomes which occur following vaccination are reported to the Vaccine Adverse Event Reporting System (VAERS)." regarding Gardasil. Dr. Russell Blaylock also discussed the low rate of reports of vaccine problems, being somewhere in the range of 2%, due to the passive and voluntary nature of the system. According to Blaylock's estimate, it is likely that there are more than 600 deaths and over 100,000 serious adverse events from this vaccine.
In analyzing the question "To vaccinate or not to vaccinate", it is important to have as much information as possible on both sides of the issue. It is easy to find arguments in support of routine vaccination against disease. The risk of catastrophic consequences from routine childhood diseases is vastly overblown. People simply don't die or endure dire consequences from these illnesses unless they are denied routine medical care for infections and encephalopathy.
"These (statistics) are designed to show maximum possible damage from the disease and minimum possible damage from the vaccine...one in a million, for instance, is the figure currently bandied about for serious reactions from the MMR vaccine. In 1991 the population of Ohio was 2,819,00 and claims from injuries from the MMR were 16..that is 1 in 176,187...with under 5 children it was 1 in 49,750...Hardly 1 in 1 million!"--
The history of the past 30 years has shown no deaths from the diseases themselves, few complications, and minimal outbreaks of the diseases that are supposed to devastate an unvaccinated population among the developed countries. Rather, the history shows striking growth in deaths and complications caused by vaccines. The saddest part of all is that the vaccines don't even do what they are claimed to do...prevent specific diseases. Instead, they can be absolutely proven to cause those diseases.
There is no convincing scientific evidence that mass inoculations can be credited with eliminating any childhood disease.
(10) It's all about increasing corporate profits. Where we are today is just the beginning.
Global annual vaccine market revenues are small compared to the overall pharmaceutical market. On the other hand, the GROWTH in the vaccine portion of the pharmaceutical market has outpaced overall growth within the sector by 200%.
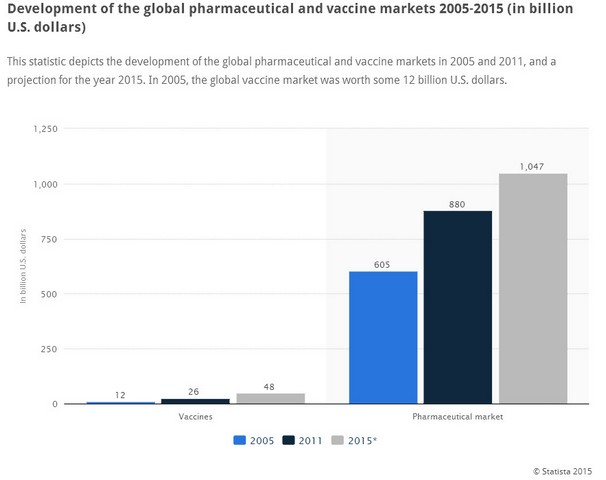
Above: Global pharmaceutical market does not quite double from 2005 to 2015
from $605 billion to $1,045 billion (i.e. just over $1 trillion)
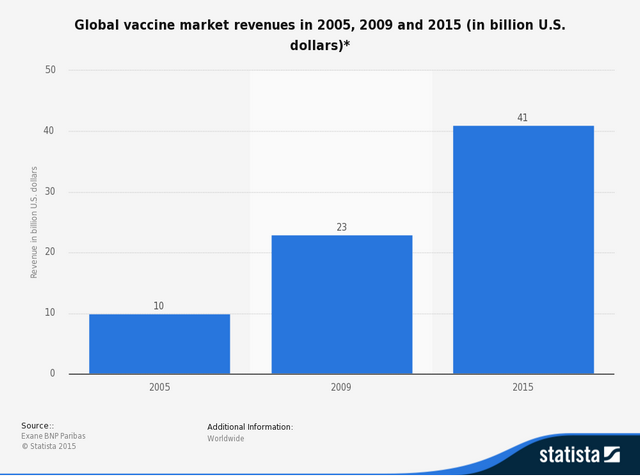
Above: Vaccine sales quadruple from 2005 to 2015 from $10 billion to $41 billion
In ten years, the vaccine market has quadrupled, outpacing its parent market by 200%. Furthermore, the pharmaceutical companies do have a plan to spur that growth rate. By frightening the general public into a panic over "preventable" diseases, they will soon convince the US lawmakers on the state level to make vaccinations mandatory in order for children to partake of public education...and possibly charter schools as well. With their control over the media by way of overall pharmaceutical advertising revenue, they will make sure that adults are aware that they must be vaccinated throughout their lives in order to have immunity to diseases that they'd have had for their entire lifetimes anyway, if only they'd undergone routine childhood diseases.
Then there are new disease threats like Ebola and human papilloma virus to make us worry about. Homeland security will probably see to it that other "terrorist" threats will come about, too. There is no telling what super bugs are lurking in chemistry labs at home and abroad. Plenty of profit in that scenario.
However, the mother lode of sector growth is still waiting in the wings. It is the Global Health Security Agenda. This is a plan to "protect at least 4 billion persons around the globe from infectious diseases." The US unveiled this plan on Feb. 13, 2014 at the peak of the Ebola virus scare. It calls for the vaccination of every child on the planet for a wide variety of diseases.
The desired impact would be "effective protection through achievement and maintenance of immunization against measles and other epidemic-prone vaccine-preventable diseases (VPDs). Measles immunization is emphasized here because it is widely recognized as a proxy indicator for overall immunization against VPDs. Countries will also identify and target immunization to populations at risk of other epidemic-prone VPDs of national importance (e.g., cholera, Japanese encephalitis, meningococcal disease, typhoid, and yellow fever). In the case of some diseases that are transferable from cattle to humans, such as anthrax and rabies, animal immunization should also be taken into account.
Participating nations so far are: Australia, Azerbaijan, Canada, Chile, China, Denmark, Ethiopia, Finland, France, Georgia, Germany, Guinea, India, Indonesia, Israel, Italy, Japan, Jordan, Kenya, Liberia, Malaysia, Mexico, Netherlands, Norway, Pakistan, Peru, Portugal, Republic of Korea, Saudi Arabia, Sierra Leone, Singapore, South Africa, Spain, Sweden, Switzerland, Thailand, Turkey, Uganda, Ukraine, United Arab Emirates, United Kingdom, United States, Vietnam, and Yemen."
It does seem as if there is unlimited potential for growth.
(11) There is a joint effort of corporations and government to cover up these facts
A heated debate is going on regarding the causality between vaccines, such as measles and anti-hepatitis B virus (HBV), and multiple sclerosis (MS). Brain antibodies as well as clinical symptoms have been found in patients vaccinated against those diseases. Other autoimmune illnesses have been associated with vaccinations. Tetanus toxoid, influenza vaccines, polio vaccine, and others, have been related to phenomena ranging from autoantibodies production to full-blown illness (such as rheumatoid arthritis (RA). Some autoimmune phenomena are clearly related to immunization (e.g. Guillain-Barre syndrome). - National Institues of Health
Did you get that? According to the US National Institutes of Health, "a heated debate is going on" in the scientific community as to the dangers of being routinely vaccinated. Why is this not breaking through to the public via our ever vigilant media?
Don't ask your doctor about the dangers of vaccines, because physicians are indoctrinated in the conventional view on these matters. They rely on statements from the United States Centers for Disease Control and Prevention (CDC). Your doctor believes in the CDC's disclaimer with its recommendations: "CDC, our planners, and our content experts wish to disclose they have no financial interests or other relationships with the manufacturers of commercial products . . . CDC does not accept commercial support."
The following is from the British Medical Journal (BMJ):
"Funding of CDC took a turn in 1983, when the CDC was authorised to accept external "gifts" from industry and other private parties. In 1992, Congress passed legislation to encourage relationships between industry and the CDC by creating the non-profit CDC Foundation, which began operations in 1995.
The CDC Foundation raised $52m in fiscal year 2014, of which $12m was from corporations. The CDC itself in fiscal year 2014 received $16m in conditional funding from sources such as corporations, individuals, and philanthropy, including the CDC Foundation. Conditional donations are earmarked for specific projects. For example, in 2012, Genentech earmarked $600,000 in donations to the CDC Foundation for CDC's efforts to promote expanded testing and treatment of viral hepatitis. Genentech and its parent company, Roche, manufacture test kits and treatments for hepatitis C.
Numerous manufacturers give donations to the CDC Foundation. Janssen also contributed $1.5m in 2012-13, and in 2011-12 contributors included Merck ($915,149), Genzyme ($762,000), Sanofi-Aventis ($600,000), and Abbott Laboratories ($550,000)." [LINK]
Other sources of information widely used by physicians are medical journals such as Journal of the American Medical Association, New England Journal of Medicine and Lancet. Again I quote from BMJ:
"Physicians and the public rely on journals as unbiased and independent sources of information and to provide leadership to improve trust in medicine and the medical literature. Yet financial conflicts of interest have repeatedly eroded the credibility of both the medical profession and journals." [LINK]
Example:
The CDC documents from Congress and discussions that [Hooker] had with the whistleblower reveal widespread manipulation of scientific data and top-down pressure on CDC scientists to support fraudulent application of government policies on vaccine safety. Based on raw data used in the 2004 DeStefano et al study obtained under the Freedom Of Information Act, Dr. Hooker found that the link between MMR vaccination and autism in African-American boys was obscured by the introduction of irrelevant and unnecessary birth certificate criteria—ostensibly to reduce the size of the study. [LINK]
Merck pharmaceutical company prosecuted for fraud over MMR vaccine
Merck & Co., one of the world's largest pharmaceutical companies, has been faking evidence of the MMR vaccine's effectiveness since at least 1997. They are currently facing federal charges brought by the US government, who is the largest single purchaser of that vaccine. The company is facing allegations of wrongdoing from different parties in the medical field, including two former Merck scientists-turned-whistleblowers. A third whistleblower, this one a scientist at the Centers for Disease Control, has joined the battle following his confession of misconduct involving the same MMR vaccine.
The following is from the independent Courthouse News Service:
Merck has known for a decade that its mumps vaccine is "far less effective" than it tells the government, and it falsified test results and sold millions of doses of "questionable efficacy," flooding and monopolizing the market, a primary caregiver claims in a federal antitrust class action.
"As the largest single purchaser of childhood vaccines (accounting for more than 50 percent of all vaccine purchases), the United States is by far the largest financial victim of Merck's fraud," according to the 2010 False Claims Act complaint. "But the ultimate victims here are the millions of children who every year are being injected with a mumps vaccine that is not providing them with an adequate level of protection. And while this is a disease that, according to the Centers for Disease Control ('CDC'), was supposed to be eradicated by now, the failure in Merck's vaccine has allowed this disease to linger, with significant outbreaks continuing to occur."
Merck is the only manufacturer licensed by the FDA to sell the mumps vaccine in United States, and if it could not show that the vaccine was 95 percent effective, it risked losing its lucrative monopoly, according to the complaint.
The only manufacturer licensed to sell the MMR vaccine in the USA has been covering up evidence of its ineffectiveness in collusion with the CDC and our federal government. Since 1983 it has been legal for the CDC to accept funding from the pharmaceutical companies, much of which was earmarked to pay for studies that "prove" the effectiveness of their products.
(12) Propaganda in favor of vaccinating is full of dishonesty and logical faults
Propaganda in favor of vaccinating is full of dishonesty and logical faults, showing a consistent thread that ignores scientific and legal data. It paints vaccine resisters as emotional, ignorant and superstitious.
The most blatant aspect of the propaganda against the vaccine choice movement is the besmirching of Dr. Andrew Wakefield for his role in a study conducted by him and Dr. John Walker-smith in their native Great Britain. Wakefield has become a straw man that is condemned by the entire pharmaceutical industry, and by media who are dependent upon their revenue. Dr. Wakefield is the world-renowned gastrointestinal surgeon and researcher who has been accused of fraud and fabricating studies that show a link between the MMR vaccine and bowel disease, present in many children with autism. He is the favored target of ad hominem attacks.
It all began when the parents of 12 children came to him for help. The children had Autism Spectrum Disorder symptoms coupled with bowel problems which all began shortly after they had been inoculated with the MMR vaccine. Wakefield found genotype evidence of the specific strain of measles used in the vaccine's manufacturing process in their bowels. He and Dr. John Walker-Smith published their case study findings in Lancet, a prestigious UK-based medical journal. Walker-Smith is one of the founding fathers of pediatric gastroenterology in the world, "an outstanding physician...well respected and a leader in the field" (Wakefield quote).
Dr. Wakefield is not an anti-vaccine doctor. Rather, he is a doctor interested in vaccine safety, and his studies led him (and many other researchers) to believe that there were problems with the three-combo vaccine of measles, mumps, and rubella (MMR). He did not advise his patients to stop vaccinating, but instead to vaccinate for these three diseases with single vaccines at separate times, rather than the combo all at once.
Dr. Wakefield's research regarding the MMR vaccine and its link to bowel disease and autism was originally published in Lancet. But a journalist by the name of Brian Deer published an article in the British Medical Journal criticizing Dr. Wakefield and accusing him of fraud. As a result, his study in Lancet was retracted. Dr. Wakefield, and one of the co-authors of the retracted article, Prof. John Walker-Smith, were barred from practicing medicine by the United Kingdom's General Medical Council regulatory board.
The thirteen original co-authors of the 1998 Lancet case study were members of the Royal Free Hospital's Inflammatory Bowel Disease Study Group. In 2004, under pressure from the British medical establishment, ten of the co-authors signed a letter retracting an interpretation of the paper that it proved that vaccines caused autism, which the paper never actually claimed in the first place. John Walker-Smith, Andrew Wakefield and Dr. Simon Murch were subsequently brought up on misconduct charges before the UK's General Medical Council. The proceedings resulted in Walker-Smith and Wakefield being found guilty and being "struck off" the medical register, while Dr. Murch retained his status as a physician. Wakefield was then vilified by corporate media and by bloggers eager to repeat scandal and engage in industry protectionism, rather than investigate the complicated facts of the story.
Wakefield, in the meantime, lost his career and name for simply following the truth his research led him to. He became the scapegoat, the "straw man" to knock down in the mainstream media. Every time someone brings up any question regarding vaccines and autism you will usually encounter something like: "That theory has been totally proven false, and the guy who made it up was convicted of fraud."
The big news is that after 16 years, Wakefield has been vindicated. Of course, you will not hear of it in mainstream media. In a stunning reversal, world renowned pediatric gastroenterologist Prof. John Walker-Smith won his appeal against the United Kingdom's General Medical Council (GMC) regulatory board that had ruled against both him and Andrew Wakefield for their roles in the 1998 Lance MMR paper, which raised questions about a link to autism. The complete victory means that Walker-Smith has been returned to the status of a fully licensed physician in the UK, although he had already retired in 2001 — six years before the GMC trial even began. Unfortunately, Wakefield did not have the financial means to challenge the UK ruling, unlike Walker-Smith whose appeal was covered by insurance. So Wakefield moved to the USA where he has continued his defense and his research.
In 1998 Lancet published that case series on twelve children receiving treatment for bowel dysfunction at the Royal Free Hospital in London. The paper called for further study of a POSSIBLE association between bowel disease and developmental delay, including cases of autism. It also noted that eight of the children's gastrointestinal and autistic symptoms began shortly after they received the MMR vaccination. The verdict today raises questions about whether or not Lancet should have retracted the paper after the GMC decision, as the reasons for its retraction have now been contradicted by the judge's decision.

Learn more: http://www.naturalnews.com/035513_Andrew_Wakefield_vaccines_autism.html#ixzz3fiiU6fWt
The false" discredited research" claims were first made in The Sunday Times of London. The result of The Sunday Times "journalism" — republished wrongfully around the world ever since — has been that hundreds of thousands of children suffering these medical conditions are being denied the medical help they need, but which is available. The overall boss for The Sunday Times, James Murdoch, CEO of News International, is also on the Board of MMR vaccine supplier and litigation defendant GlaxoSmithKline. Murdoch's Glaxo job is expressly to oversee"external issues that might have the potential for serious impact upon the group's business and reputation" ["James Murdoch takes GlaxoSmithKline role" - Chris Tryhorn The Guardian Monday 2 February 2009.]
Fronted by London Times reporter Brian Deer. The Times is owned by publishing magnate Rupert Murdoch, and run by his son, James. The junior Murdoch is on the board of directors of Glaxo-Smith-Kline, maker of the MMR vaccine. Deer used a private investigating firm, Medico-Legal Investigations, to research his story. The firm's sole source of funding was the Association of the British Pharmaceutical Industry. Deer was both the journalist writing on Wakefield and the person who brought a case of fitness to practice medicine to the General Medical Council, and then wrote about the proceedings as well.
More Glaxo-Smith-Kline connections came into play. The parents of the children involved in Wakefield's study have never wavered in their support of him. They wanted to be heard during the proceedings against him. They were denied that right by High Court judge Sir Nigil Davis, whose brother is on the Executive Board of Lancet and the Board of Directors of...you guessed it...Glaxo-Smith-Kline.
If you look up the Wikepedia article on Wakefield, you will discover a blatantly false telling of the whole affair. The first sentence reads:
"Andrew Jeremy Wakefield (born 1957) is a British former gastroenterologist and medical researcher who was struck off the UK medical register for his fraudulent 1998 research paper, and other proven charges of misconduct, in support of the now-discredited claim that there was a link between the administration of the measles, mumps and rubella (MMR) vaccine, and the appearance of autism and bowel disease."
This pack of lies leads to a Time Magazine article called Great Science Frauds. In it he is tarred-and-feathered with statements totally lacking in substantiation that treat the whole matter of harms caused by vaccine as completely unproven.
CONCLUSION
The medical establishment got it all in reverse: it is not vaccine-exempt children who endanger us all, it is the effects of prolonged mass-vaccination campaigns that have done so. When would the medical establishment (and the media) start paying attention to the long-term consequences of mass-vaccination measures instead of hastily and unjustifiably blaming every outbreak on the unvaccinated? Tetyana Obukhanych, PhD Immunology
"Show us the science, and give us the choice"
The next time you visit your doctor, after your doctor is done telling you how safe vaccines are, ask him or her this question with the 9 magic words: "If this vaccine injures my child, who is responsible?"
Your doctor will likely blush, get angry with you, or avoid the question altogether. What the doctor will avoid telling you is that vaccines are inherently unsafe! This means that even if vaccines are handled and given properly, some children will die or will be hurt. If you doubt that, ask for the package insert before you agree to vaccination.
The reality — and the answer to the question — is this: You are responsible if your child is injured!
________________________________________________________________________________________
Recommended links –
Former Merck Rep Says Mandatory Vaccination Is For Profit and Not Public Health (9 min 41 sec)
https://www.youtube.com/watch?v=d1sM7RXz0JI
Silent Epidemic: The Untold Story of Vaccines directed by Gary Null (1 hr 48 min)
https://www.youtube.com/watch?v=iQ_2BVsfdgI
Vaccines & Brain Development Dr. Russell Blaylock (1 hr 28 min) [Author's note: This is a lecture Blaylock did for Radio Liberty, a right wing organization. In it he makes a few political comments. Ignore them; his scientific knowledge is above reproach]
https://www.youtube.com/watch?v=JjVR12DZ2oI
________________________________________________________________________________________
CHANGES.
1. Ryan Mojabi link to settlement amount
2. Former Merck Rep admits motive link immediately above this list